Viderman Dmitriy, Aubakirova Mina, Umbetzhanov Yerlan, Kulkaeva Gulnara, Shalekenov S B, Abdildin Yerkin G
Nazarbayev University School of Medicine (NUSOM), Nur-Sultan, Kazakhstan.
National Research Oncology Center, Nur-Sultan, Kazakhstan.
Front Med (Lausanne). 2022 Jul 4;9:932101. doi: 10.3389/fmed.2022.932101. eCollection 2022.
Neurosurgical spinal surgeries such as micro- discectomy and complex fusion surgeries remain the leading causes of disability-adjusted life-year. Major spinal surgeries often result in severe postprocedural pain due to massive dissection of the underlying tissues. While opioids offer effective pain control, they frequently lead to side effects, such as post-operative nausea and vomiting, pruritus, constipation, and respiratory depression. ESPB was successfully used in spinal surgery as a component of a multimodal analgesic regimen and it eliminated the requirements for opioids. The primary purpose of this systematic review and meta-analysis was to compare post-operative opioid consumption between ESPB and placebo.
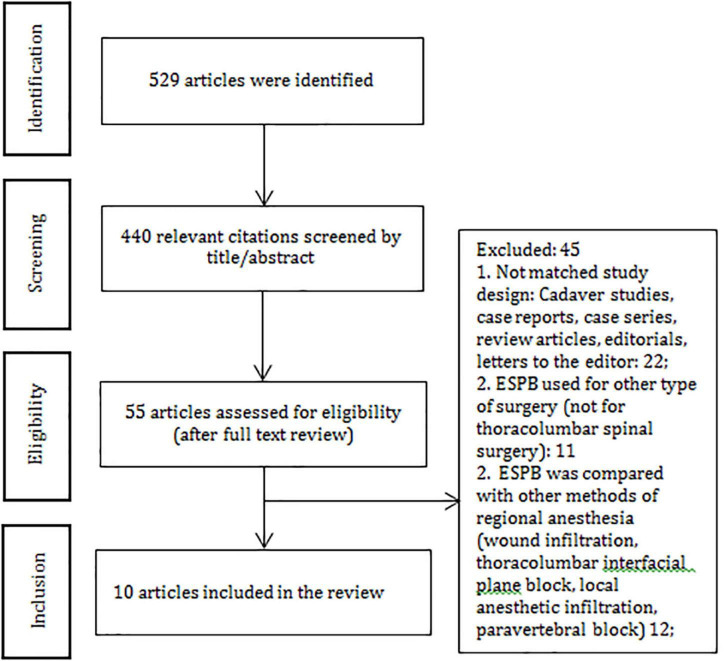
To conduct this systematic review, we used the "Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)" guidelines. We conducted a search for relevant articles available in the following databases: Google Scholar, PubMed, and the Cochrane Library published up to March 2022.
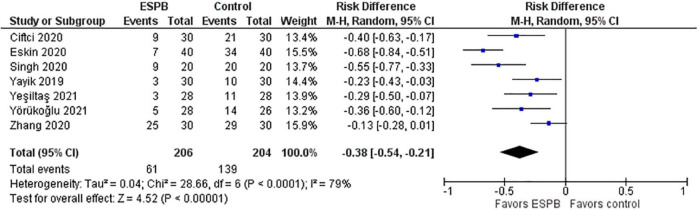
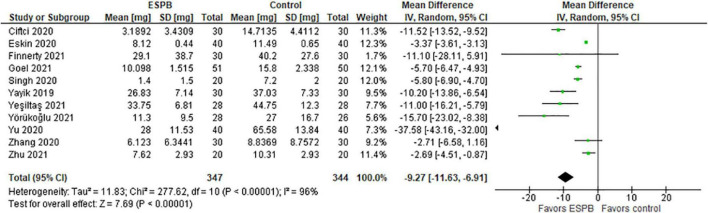
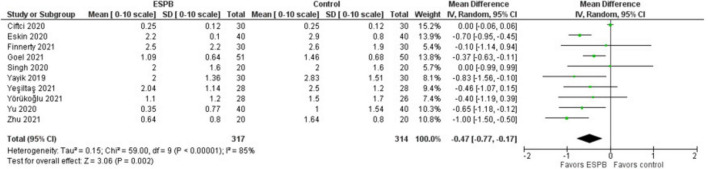
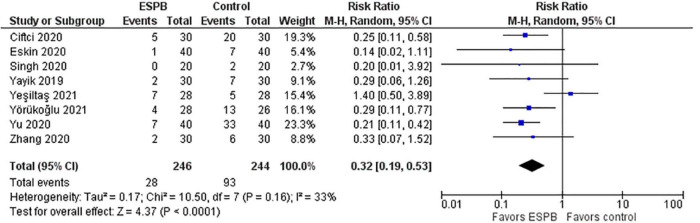
The total morphine consumption within 24 h after surgery was lower in the ESPB group, the mean difference (in mg of morphine) with 95% CI is -9.27 (-11.63, -6.91). The pain intensity (0-10) at rest measured 24 h after surgery was lower in the ESPB group, the MD with 95% CI is -0.47 (-0.77, -0.17). The pain intensity during movement measured 24 h after surgery was lower in the ESPB group, the MD with 95% CI is -0.73 (-1.00, -0.47). Post-operative nausea and vomiting were significantly lower in the ESPB group, the risk ratio with 95% CI is 0.32 (0.19, 0.53).
Ultrasound-guided ESPB was superior to placebo in reducing post-operative opioid consumption, pain intensity, post-operative nausea and vomiting, and prolonging the time to first rescue analgesia. There were no ESPB-related serious complications reported.
神经外科脊柱手术,如显微椎间盘切除术和复杂融合手术,仍然是导致残疾调整生命年的主要原因。大型脊柱手术由于对深层组织的大量解剖,术后常导致严重疼痛。虽然阿片类药物能有效控制疼痛,但它们经常会引发副作用,如术后恶心、呕吐、瘙痒、便秘和呼吸抑制。椎旁肌间隙阻滞(ESPB)作为多模式镇痛方案的一部分,已成功应用于脊柱手术,且无需使用阿片类药物。本系统评价和荟萃分析的主要目的是比较ESPB与安慰剂术后阿片类药物的消耗量。
为进行本系统评价,我们采用了“系统评价和荟萃分析的首选报告项目(PRISMA)”指南。我们在以下数据库中搜索了截至2022年3月发表的相关文章:谷歌学术、PubMed和考克兰图书馆。
ESPB组术后24小时内的吗啡总消耗量较低,平均差值(吗啡毫克数)及95%置信区间为-9.27(-11.63,-6.91)。ESPB组术后24小时静息时的疼痛强度(0-10分)较低,平均差值及95%置信区间为-0.4(-0.77,-0.17)。ESPB组术后24小时活动时的疼痛强度较低,平均差值及95%置信区间为-0.73(-1.00,-0.47)。ESPB组术后恶心和呕吐明显较少,风险比及95%置信区间为0.32(0.19,0.53)。
超声引导下的ESPB在减少术后阿片类药物消耗量、疼痛强度、术后恶心和呕吐以及延长首次补救镇痛时间方面优于安慰剂。未报告与ESPB相关的严重并发症。