Rabinowitz Keren Masha, Navon Michal, Edelman-Klapper Hadar, Zittan Eran, Bar-Gil Shitrit Ariella, Goren Idan, Avni-Biron Irit, Ollech Jacob E, Lichtenstein Lev, Banai-Eran Hagar, Yanai Henit, Snir Yifat, Pauker Maor H, Friedenberg Adi, Levy-Barda Adva, Segal Arie, Broitman Yelena, Maoz Eran, Ovadia Baruch, Aharoni Golan Maya, Shachar Eyal, Ben-Horin Shomron, Maharshak Nitsan, Mor Michal, Ben Zvi Haim, Eliakim Rami, Barkan Revital, Sharar-Fischler Tali, Goren Sophy, Krugliak Noy, Pichinuk Edward, Mor Michael, Werbner Michal, Alter Joel, Abu-Taha Hanan, Kaboub Kawsar, Dessau Moshe, Gal-Tanamy Meital, Cohen Dani, Freund Natalia T, Dotan Iris
Division of Gastroenterology, Rabin Medical Center, Petah Tikva 4941492, Israel.
Felsenstein Medical Research Center, Sackler School of Medicine, Tel Aviv 69978, Israel.
Vaccines (Basel). 2022 Jul 26;10(8):1186. doi: 10.3390/vaccines10081186.
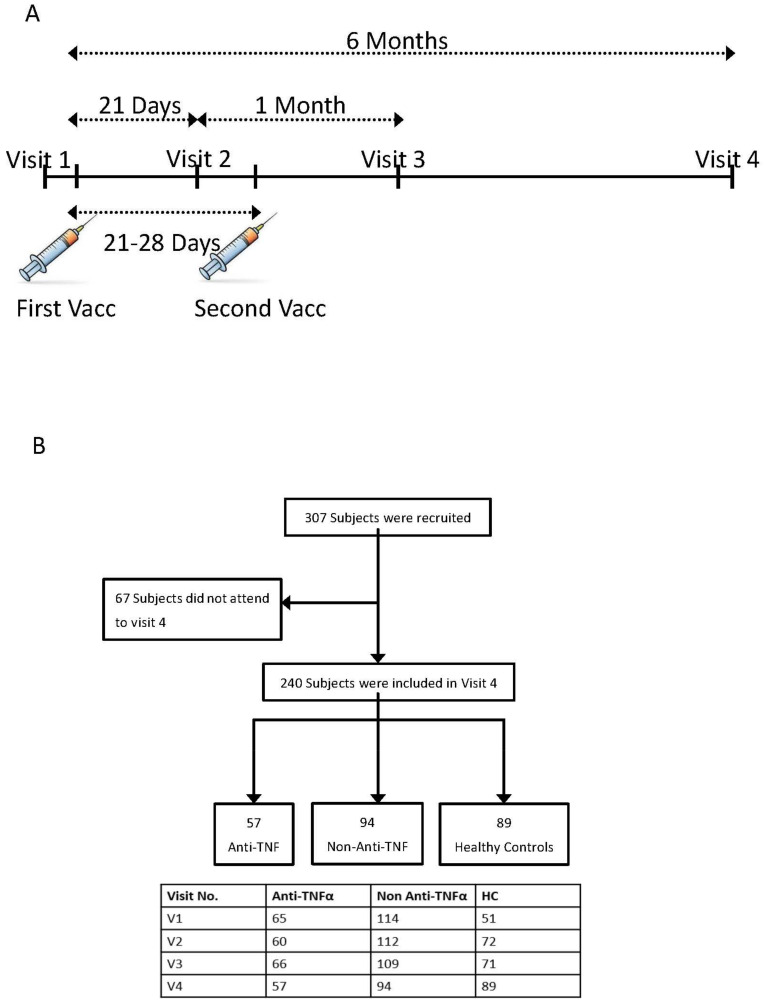
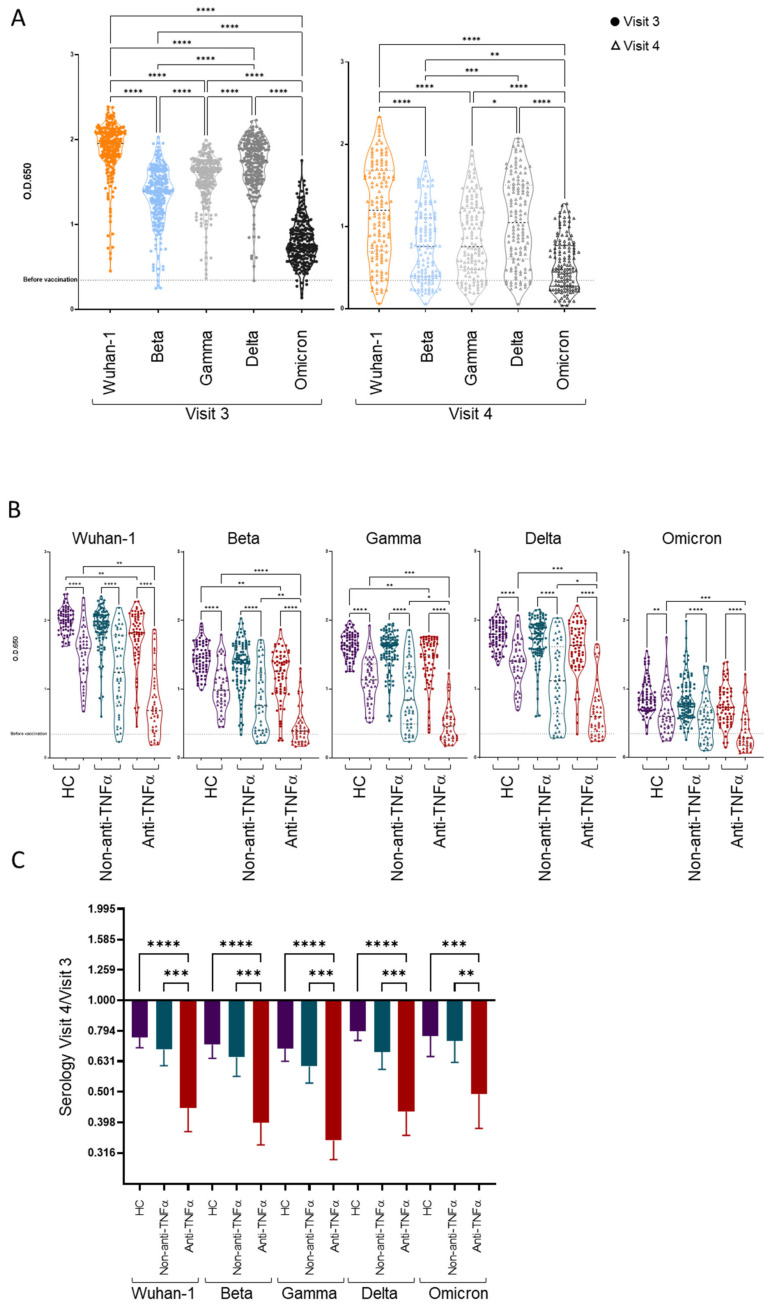
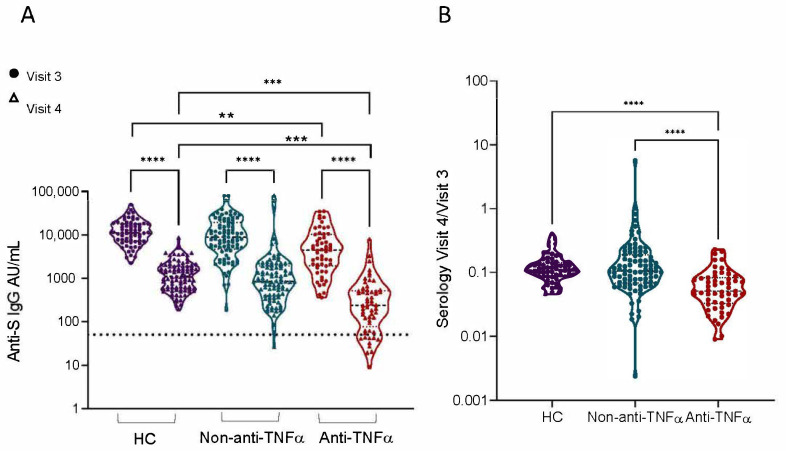
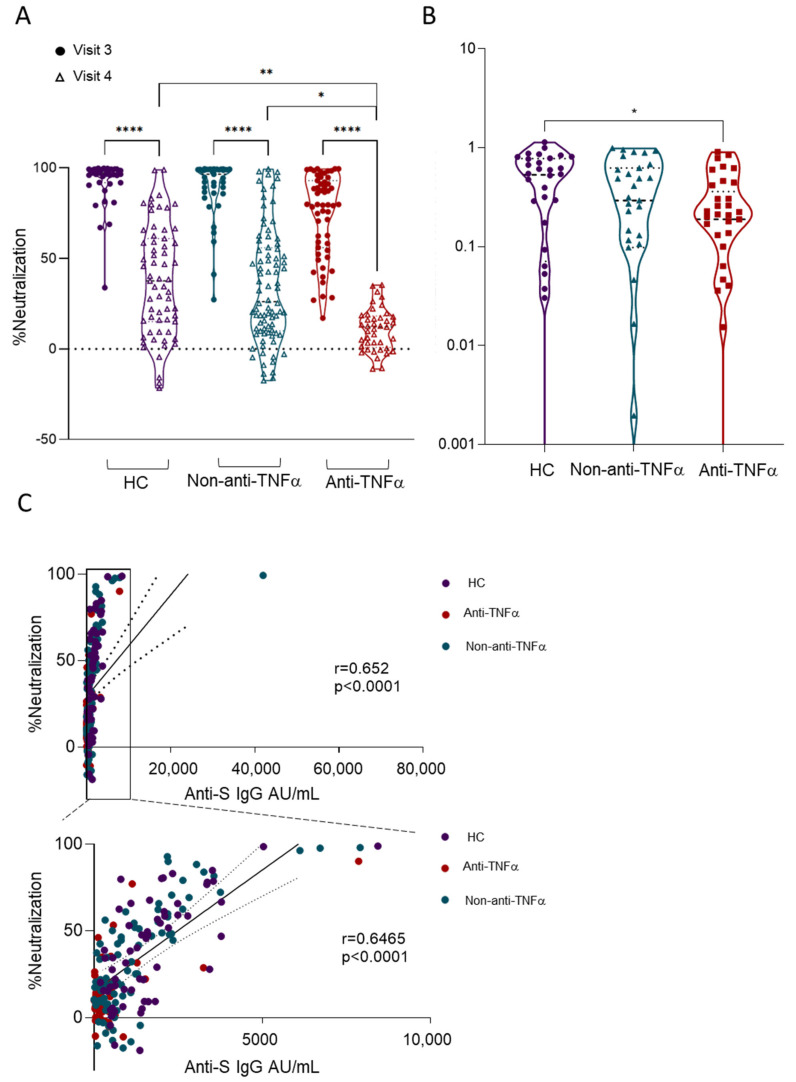
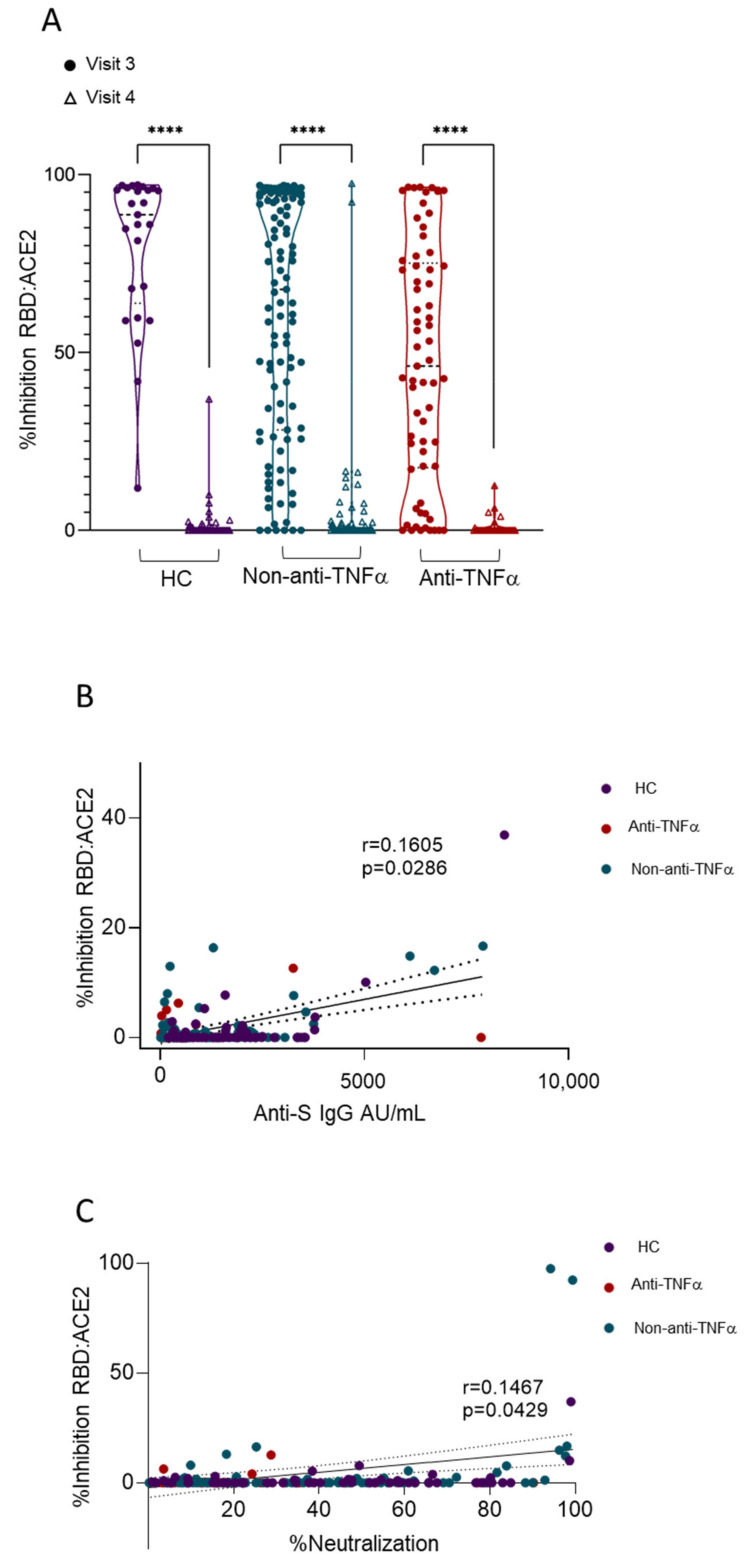
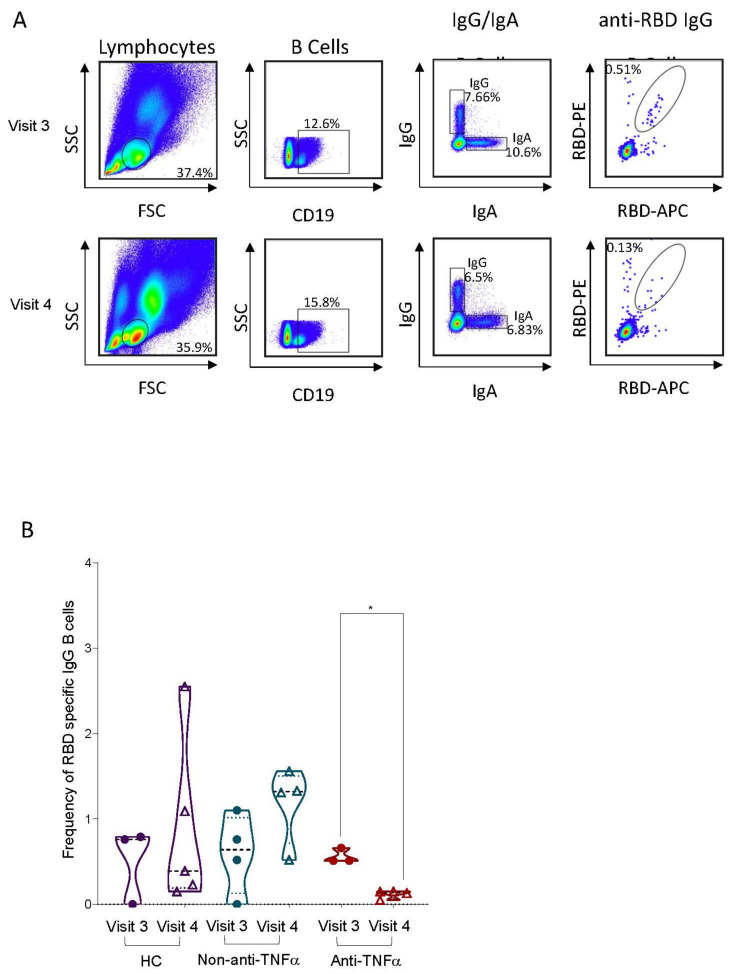
Patients with inflammatory bowel disease (IBD) treated with anti-tumor-necrosis factor-alpha (TNFα) exhibited lower serologic responses one-month following the second dose of the COVID-19 BNT162b2 vaccine compared to those not treated with anti-TNFα (non-anti-TNFα) or to healthy controls (HCs). We comprehensively analyzed long-term humoral responses, including anti-spike (S) antibodies, serum inhibition, neutralization, cross-reactivity and circulating B cell six months post BNT162b2, in patients with IBD stratified by therapy compared to HCs. Subjects enrolled in a prospective, controlled, multi-center Israeli study received two BNT162b2 doses. Anti-S levels, functional activity, specific B cells, antigen cross-reactivity, anti-nucleocapsid levels, adverse events and IBD disease score were detected longitudinally. In total, 240 subjects, 151 with IBD (94 not treated with anti-TNFα and 57 treated with anti-TNFα) and 89 HCs participated. Six months after vaccination, patients with IBD treated with anti-TNFα had significantly impaired BNT162b2 responses, specifically, more seronegativity, decreased specific circulating B cells and cross-reactivity compared to patients untreated with anti-TNFα. Importantly, all seronegative subjects were patients with IBD; of those, >90% were treated with anti-TNFα. Finally, IBD activity was unaffected by BNT162b2. Altogether these data support the earlier booster dose administration in these patients.
与未接受抗肿瘤坏死因子-α(TNFα)治疗的患者(非抗TNFα组)或健康对照(HCs)相比,接受抗TNFα治疗的炎症性肠病(IBD)患者在接种第二剂COVID-19 BNT162b2疫苗后1个月时血清学反应较低。我们全面分析了BNT162b2接种后6个月时IBD患者的长期体液反应,包括抗刺突(S)抗体、血清抑制、中和、交叉反应性和循环B细胞,并与HCs进行了分层治疗比较。参加以色列一项前瞻性、对照、多中心研究的受试者接受了两剂BNT162b2。纵向检测抗S水平、功能活性、特异性B细胞、抗原交叉反应性、抗核衣壳水平、不良事件和IBD疾病评分。共有240名受试者参与,其中151名IBD患者(94名未接受抗TNFα治疗,57名接受抗TNFα治疗)和89名HCs。接种疫苗6个月后,与未接受抗TNFα治疗的患者相比,接受抗TNFα治疗的IBD患者的BNT162b2反应明显受损,具体表现为更多的血清阴性、特异性循环B细胞减少和交叉反应性降低。重要的是,所有血清阴性受试者均为IBD患者;其中,>90%接受抗TNFα治疗。最后,IBD活性不受BNT162b2的影响。这些数据共同支持在这些患者中尽早给予加强剂量。