School of Allied Health, Curtin University, Bentley, Western Australia, Australia.
Monash Rural Health, Monash University, Churchill, Victoria, Australia.
PeerJ. 2022 Jul 25;10:e13627. doi: 10.7717/peerj.13627. eCollection 2022.
Many potential factors associated with Inflammatory Conditions of the Lactating Breast (ICLB) have been reported in the literature, by lactating mothers and clinicians. Clinicians, including general practitioners, lactation consultants and physiotherapists, require a clinical reasoning model that summarises associated or linked factors, to aid in the assessment, treatment, and prevention of ICLB. Thus, we aimed to adapt the existing Breastfeeding Pain Reasoning Model (BPRM), for use in the management of ICLB, using prior research and clinical audit data to guide adaptation. The existing BPRM categorises contributing factors for breastfeeding nipple pain, rather than ICLB.
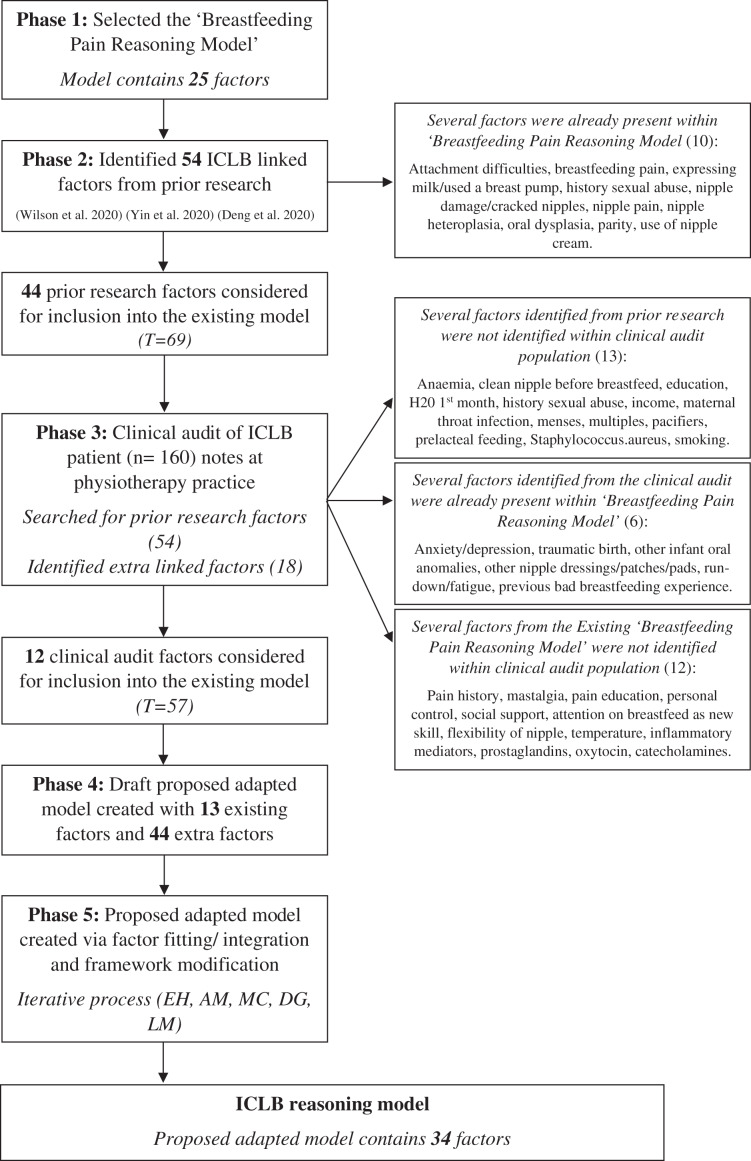
Factors linked with ICLB were identified from prior research and considered for inclusion into the existing model. Clinical data from a retrospective audit of ICLB patient notes at a private physiotherapy practice were also examined. Any factors identified from prior research that could not be identified in the clinical notes were not considered for inclusion into the existing model. Additional factors from the clinical notes that appeared repeatedly were considered for inclusion into the adaptation of the BPRM. A draft adapted model was created comprising all eligible factors, considering their counts and percentages as calculated from the clinical data. The research team iteratively examined all factors for appropriate categorisation and modification within the adapted model.
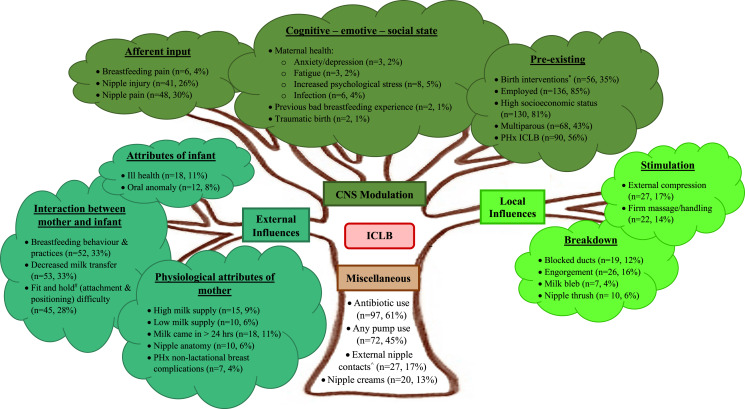
Prior research and data from 160 clinical notes were used to identify factors for inclusion in the adapted model. A total of 57 factors, 13 pre-existing in the BPRM and 44 extra identified from the prior research or clinical audit, comprised the draft adapted model. Factor consolidation and terminology modification resulted in a total of 34 factors in the final proposed adapted ICLB model. The three main categories, CNS modulation, External influences and Local stimulation, from the existing model were maintained, with one minor terminology change to the former Local stimulation category, resulting in 'Local influences' category. Terminology for five subcategories were modified to better reflect the types of factors for ICLB. The most common factors in the adapted model, calculated from the clinical audit population of mothers with ICLB, were employment (85%), high socioeconomic status (81%), antibiotic use during breastfeeding (61%), history of an ICLB (56%), any breast pump use (45%), multiparity (43%), birth interventions (35%), decreased milk transfer (33%), breastfeeding behaviour and practices (33%), nipple pain (30%) and fit and hold (attachment and positioning) difficulty (28%).
An ICLB-specific linked factors model is proposed in this paper. Clinicians treating mothers with ICLB can use this model to identify influencing and determining factors of ICLB clinical presentations and provide targeted education and effective treatment plans.
许多与哺乳期乳腺炎(ICLB)相关的潜在因素已在文献中被哺乳期母亲和临床医生报道。包括全科医生、哺乳顾问和物理治疗师在内的临床医生需要一个临床推理模型来总结相关或关联因素,以帮助评估、治疗和预防 ICLB。因此,我们旨在使用先前的研究和临床审计数据来指导改编,改编现有的母乳喂养疼痛推理模型(BPRM),以用于 ICLB 的管理。现有的 BPRM 对导致母乳喂养乳头疼痛的因素进行了分类,而不是 ICLB。
从先前的研究中确定与 ICLB 相关的因素,并考虑将其纳入现有模型。还检查了私人物理治疗实践中对 ICLB 患者病历进行回顾性审计的临床数据。在临床记录中无法识别的先前研究中确定的任何因素均未被考虑纳入现有模型。从临床记录中反复出现的其他因素被认为是纳入 BPRM 改编的因素。创建了一个包含所有合格因素的草案改编模型,考虑了从临床数据中计算得出的计数和百分比。研究团队迭代地检查了所有因素,以在改编模型中进行适当的分类和修改。
先前的研究和 160 份临床记录的数据用于确定纳入改编模型的因素。共有 57 个因素,其中 13 个是 BPRM 中的现有因素,44 个是从先前的研究或临床审计中确定的额外因素,构成了草案改编模型。通过因素合并和术语修改,最终提出的改编 ICLB 模型中共有 34 个因素。现有的模型中的三个主要类别,即 CNS 调节、外部影响和局部刺激,得到了保留,以前的局部刺激类别更名为“局部影响”类别。五个子类别术语进行了修改,以更好地反映 ICLB 的类型因素。从患有 ICLB 的母亲的临床审计人群中计算出改编模型中最常见的因素为就业(85%)、高社会经济地位(81%)、哺乳期使用抗生素(61%)、有 ICLB 病史(56%)、任何吸奶器使用(45%)、多胎(43%)、分娩干预(35%)、乳汁转移减少(33%)、母乳喂养行为和做法(33%)、乳头疼痛(30%)和贴合和握持(附接和定位)困难(28%)。
本文提出了一种与 ICLB 相关的特定关联因素模型。治疗患有 ICLB 的母亲的临床医生可以使用该模型识别影响 ICLB 临床表现的影响因素和决定因素,并提供有针对性的教育和有效的治疗计划。