From the Division of Clinical Geriatrics (N.C., D.F., A.M., J.B.P., S.S., L.-O.W., M.E., E.W.), Centre for Alzheimer Research, Department of Neurobiology, Care Sciences, and Society, and the Division of Insurance Medicine (A.M.), Department of Clinical Neuroscience, Karolinska Institutet, Stockholm; Department of Psychology (N.C.), Sensory Cognitive Interaction Laboratory (SCI-lab), Stockholm University, Sweden; Department of Radiology (D.F.), Mayo Clinic, Rochester, MN; Department of Cybernetics (M.N.), Faculty of Electrical Engineering and Czech Institute of Informatics (M.N., O.S., L.V.), Robotics, and Cybernetics, Czech Technical University, Prague, Czech Republic; Clinical Memory Research Unit (J.B.P.), Department of Clinical Sciences, Lund University, Malmö; Department of Psychiatry Cognition and Old Age Psychiatry, (A.Z., S.K., I.S.), Clinical Neurochemistry Laboratory (K.B., H.Z.), and Department of Clinical Physiology (M.S.), Sahlgrenska University Hospital, Gothenburg; Neuropsychiatric Epidemiology Unit (A.Z., K.B., H.Z., S.K., I.S.), Department of Psychiatry and Neurochemistry, Institute of Neuroscience and Physiology, the Sahlgrenska Academy, Centre for Ageing and Health (AGECAP) at the University of Gothenburg; Theme Inflammation and Aging (M.E.), Karolinska University Hospital, Huddinge, Sweden; Clinical Dementia Research Section (S.T.), Department of Psychosomatic Medicine, University Medicine Rostock; German Center for Neurodegenerative Diseases (DZNE) (S.T., M.J.G.), Rostock, Germany; Unidad de Trastornos del Movimiento (M.J.G.), Servicio de Neurología y Neurofisiología Clínica, Instituto de Biomedicina de Sevilla (IBiS), Hospital Universitario Virgen del Rocío/CSIC/Universidad de Sevilla, Spain; Department of Neurodegenerative Disease (H.Z.), UCL Institute of Neurology, London; Dementia Research Institute at UCL (H.Z.), London, UK; Hong Kong Center for Neurodegenerative Diseases (H.Z.), China; Wallenberg Centre for Molecular and Translational Medicine (M.S.) and Department of Psychiatry and Neurochemistry (M.S.), Institute of Physiology and Neuroscience, University of Gothenburg, Sweden; Dementia Research Centre (M.S.), Institute of Neurology, University College London; and Department of Neuroimaging (E.W.), Centre for Neuroimaging Sciences, Institute of Psychiatry, Psychology and Neuroscience, King's College London, UK.
Neurology. 2022 Oct 11;99(15):e1619-e1629. doi: 10.1212/WNL.0000000000200930. Epub 2022 Aug 2.
Several pathologic processes might contribute to the degeneration of the cholinergic system in aging. We aimed to determine the contribution of amyloid, tau, and cerebrovascular biomarkers toward the degeneration of cholinergic white matter (WM) projections in cognitively unimpaired individuals.
The contribution of amyloid and tau pathology was assessed through CSF levels of the Aβ ratio and phosphorylated tau (p-tau). CSF Aβ levels were also measured. Cerebrovascular pathology was assessed using automatic segmentations of WM lesions (WMLs) on MRI. Cholinergic WM projections (i.e., cingulum and external capsule pathways) were modeled using tractography based on diffusion tensor imaging data. Sex and APOE ε4 carriership were also included in the analysis as variables of interest.
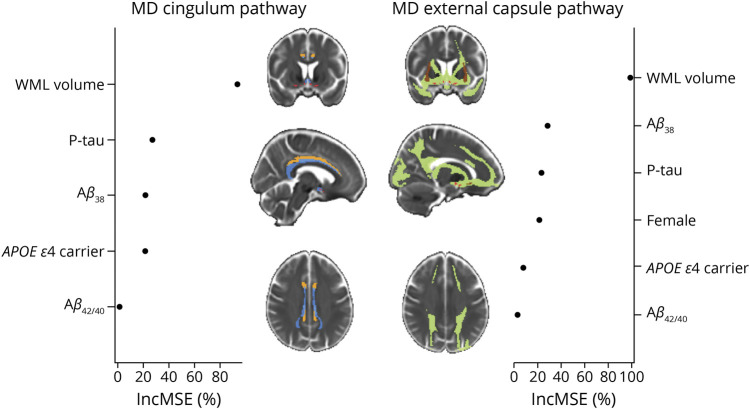
We included 203 cognitively unimpaired individuals from the H70 Gothenburg Birth Cohort Studies (all individuals aged 70 years, 51% female). WM lesion burden was the most important contributor to the degeneration of both cholinergic pathways (increase in mean square error [IncMSE] = 98.8% in the external capsule pathway and IncMSE = 93.3% in the cingulum pathway). Levels of Aβ and p-tau also contributed to cholinergic WM degeneration, especially in the external capsule pathway (IncMSE = 28.4% and IncMSE = 23.4%, respectively). The Aβ ratio did not contribute notably to the models (IncMSE<3.0%). APOE ε4 carriers showed poorer integrity in the cingulum pathway (IncMSE = 21.33%). Women showed poorer integrity of the external capsule pathway (IncMSE = 21.55%), which was independent of amyloid status as reflected by the nonsignificant differences in integrity when comparing amyloid-positive vs amyloid-negative women participants (T = -1.55; = 0.123).
In cognitively unimpaired older individuals, WMLs play a central role in the degeneration of cholinergic pathways. Our findings highlight the importance of WM lesion burden in the elderly population, which should be considered in the development of prevention programs for neurodegeneration and cognitive impairment.
多种病理过程可能导致衰老过程中胆碱能系统的退化。我们旨在确定淀粉样蛋白、tau 和脑血管生物标志物对认知正常个体胆碱能白质(WM)投射退化的贡献。
通过 CSF 中 Aβ 比值和磷酸化 tau(p-tau)的水平来评估淀粉样蛋白和 tau 病理学的贡献。还测量了 CSF 中的 Aβ 水平。使用 MRI 上 WM 病变(WML)的自动分割来评估脑血管病理学。使用基于弥散张量成像数据的轨迹法来模拟胆碱能 WM 投射(即胼胝体和外囊通路)。在分析中还包括性别和 APOE ε4 携带情况作为感兴趣的变量。
我们纳入了来自 H70 哥德堡出生队列研究的 203 名认知正常的个体(所有个体年龄均为 70 岁,女性占 51%)。WM 病变负担是两条胆碱能通路退化的最重要因素(外囊通路的平均平方误差增加[IncMSE]为 98.8%,胼胝体通路的 IncMSE 为 93.3%)。Aβ 和 p-tau 的水平也与胆碱能 WM 退化有关,尤其是在外囊通路(IncMSE 分别为 28.4%和 23.4%)。Aβ 比值对模型的贡献不显著(IncMSE<3.0%)。APOE ε4 携带者的胼胝体通路完整性较差(IncMSE = 21.33%)。女性的外囊通路完整性较差(IncMSE = 21.55%),这与淀粉样蛋白状态无关,因为在比较淀粉样蛋白阳性和阴性女性参与者时,完整性没有显著差异(T = -1.55;p = 0.123)。
在认知正常的老年人中,WML 在外囊和胼胝体通路的退化中起着核心作用。我们的研究结果强调了 WM 病变负担在老年人群中的重要性,这应该在神经退行性变和认知障碍的预防计划的制定中加以考虑。