Baldridge Abigail S, Aluka-Omitiran Kasarachi, Orji Ikechukwu A, Shedul Gabriel L, Ojo Tunde M, Eze Helen, Shedul Grace, Ugwuneji Eugenia N, Egenti Nonye B, Okoli Rosemary C B, Ale Boni M, Nwankwo Ada, Osagie Samuel, Ye Jiancheng, Chopra Aashima, Sanuade Olutobi A, Tripathi Priya, Kandula Namratha R, Hirschhorn Lisa R, Huffman Mark D, Ojji Dike B
Northwestern University Feinberg School of Medicine, Chicago, IL, USA.
Cardiovascular Research Unit, University of Abuja Teaching Hospital, Abuja, Nigeria.
Implement Sci Commun. 2022 Aug 2;3(1):84. doi: 10.1186/s43058-022-00328-9.
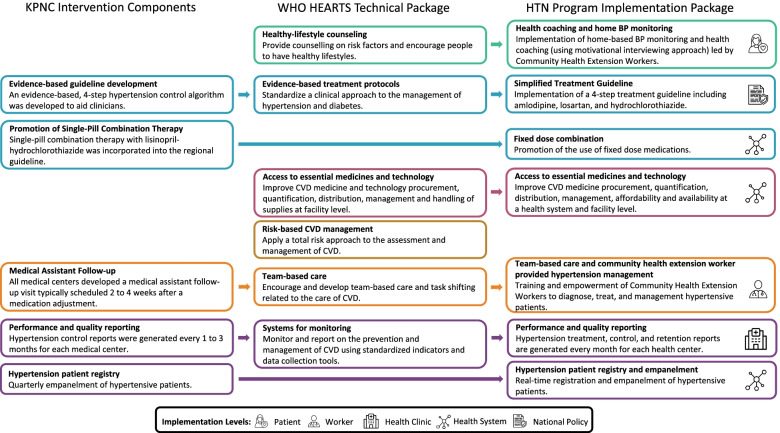
Hypertension is the most common cardiovascular disease in Nigeria and contributes to a large non-communicable disease burden. Our aim was to implement and evaluate a large-scale hypertension treatment and control program, adapted from the Kaiser Permanent Northern California and World Health Organization HEARTS models, within public primary healthcare centers in the Federal Capital Territory, Nigeria.
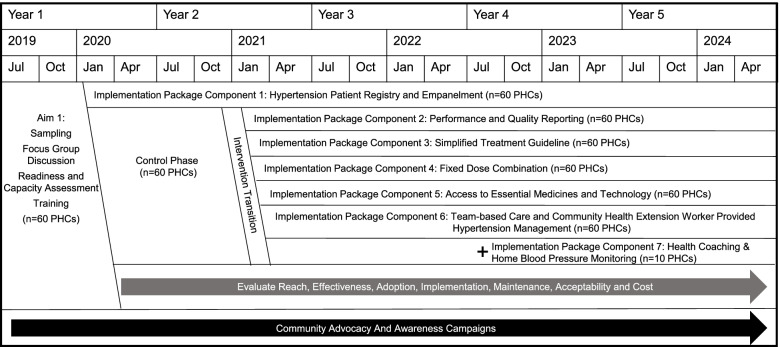
A type 2 hybrid, interrupted time series design was used to generate novel information on large-scale implementation and effectiveness of a multi-level hypertension control program within 60 primary healthcare centers in the Federal Capital Territory, Nigeria. During the formative phase, baseline qualitative assessments were held with patients, health workers, and administrators to inform implementation package adaptation. The package includes a hypertension patient registry with empanelment, performance and quality reporting, simplified treatment guideline emphasizing fixed-dose combination therapy, reliable access to quality essential medicines and technology, team-based care, and health coaching and home blood pressure monitoring. Strategies to implement and adapt the package were identified based on barriers and facilitators mapped in the formative phase, previous implementation experience, mid-term qualitative evaluation, and ongoing stakeholder and site feedback. The control phase included 11 months of sequential registration of hypertensive patients at participating primary healthcare centers, followed by implementation of the remainder of the package components and evaluation over 37 subsequent, consecutive months of the intervention phase. The formative phase was completed between April 2019 and August 2019, followed by initiation of the control phase in January 2020. The control phase included 11 months (January 2020 to November 2020) of sequential registration and empanelment of hypertensive patients at participating primary healthcare centers. After completion of the control phase in November 2020, the intervention phase commenced in December 2020 and will be completed in December 2023.
This trial will provide robust evidence for implementation and effectiveness of a multi-level implementation package more broadly throughout the Federal Capital Territory, which may inform hypertension systems of care throughout Nigeria and in other low- and middle-income countries. Implementation outcome results will be important to understand what system-, site-, personnel-, and patient-level factors are necessary for successful implementation of this intervention.
ClinicalTrials.gov NCT04158154 . The trial was prospectively registered on November 8, 2019.
高血压是尼日利亚最常见的心血管疾病,导致了巨大的非传染性疾病负担。我们的目标是在尼日利亚联邦首都地区的公共初级卫生保健中心实施并评估一项大规模高血压治疗与控制项目,该项目改编自北加利福尼亚凯撒医疗集团和世界卫生组织的HEARTS模式。
采用2型混合中断时间序列设计,以获取有关尼日利亚联邦首都地区60家初级卫生保健中心内多层次高血压控制项目大规模实施情况及有效性的新信息。在形成阶段,对患者、卫生工作者和管理人员进行了基线定性评估,以为实施方案的调整提供依据。该方案包括一个高血压患者登记册,涵盖入组、绩效和质量报告,强调固定剂量联合治疗的简化治疗指南,可靠获取优质基本药物和技术,团队式护理,以及健康指导和家庭血压监测。根据形成阶段确定的障碍和促进因素、以往的实施经验、中期定性评估以及利益相关者和各站点的持续反馈,确定了实施和调整该方案的策略。对照阶段包括在参与的初级卫生保健中心对高血压患者进行11个月的连续登记,随后实施该方案的其余组成部分,并在随后连续37个月的干预阶段进行评估。形成阶段于2019年4月至2019年8月完成,随后于2020年1月开始对照阶段。对照阶段包括在参与的初级卫生保健中心对高血压患者进行11个月(2020年1月至2020年11月)的连续登记和入组。2020年11月完成对照阶段后,干预阶段于2020年12月开始,并将于2023年12月完成。
该试验将为在整个联邦首都地区更广泛地实施多层次实施方案及其有效性提供有力证据,这可能为尼日利亚及其他低收入和中等收入国家的高血压护理系统提供参考。实施结果对于了解成功实施该干预措施所需的系统、站点、人员和患者层面的因素非常重要。
ClinicalTrials.gov NCT04158154 。该试验于2019年11月8日进行前瞻性注册。