Migliore Federico, Martini Nicolò, Calo' Leonardo, Martino Annamaria, Winnicki Giulia, Vio Riccardo, Condello Chiara, Rizzo Alessandro, Zorzi Alessandro, Pannone Luigi, Miraglia Vincenzo, Sieira Juan, Chierchia Gian-Battista, Curcio Antonio, Allocca Giuseppe, Mantovan Roberto, Salghetti Francesca, Curnis Antonio, Bertaglia Emanuele, De Lazzari Manuel, de Asmundis Carlo, Corrado Domenico
Department of Cardiac, Thoracic, Vascular Sciences and Public Health, University of Padova, Padova, Italy.
Department of Cardiology, Policlinico Casilino, Rome, Italy.
Front Cardiovasc Med. 2022 Jul 22;9:964694. doi: 10.3389/fcvm.2022.964694. eCollection 2022.
Predictors of late life-threatening arrhythmic events in Brugada syndrome (BrS) patients who received a prophylactic ICD implantation remain to be evaluated. The aim of the present long-term multicenter study was to assess the incidence and clinical-electrocardiographic predictors of late life-threatening arrhythmic events in BrS patients with a prophylactic implantable cardioverter defibrillator (ICD) and undergoing generator replacement (GR).
The study population included 105 patients (75% males; mean age 45 ± 14years) who received a prophylactic ICD and had no arrhythmic event up to first GR.
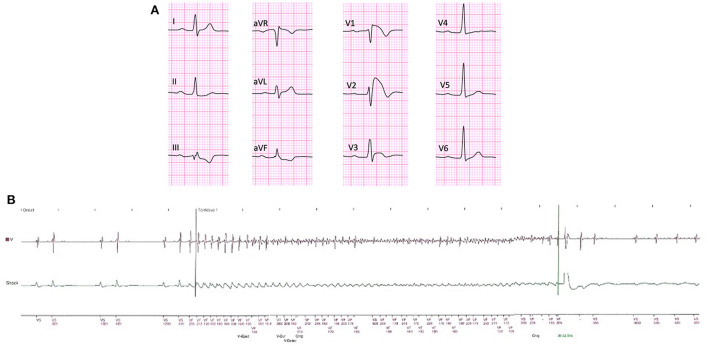
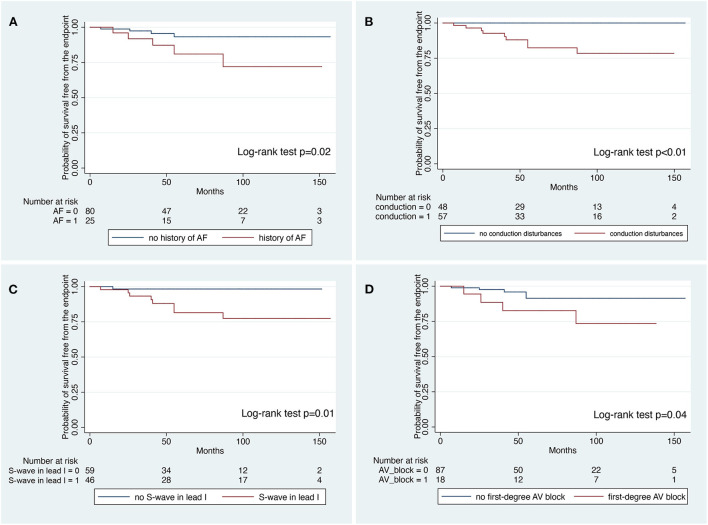
The median period from first ICD implantation to last follow-up was 155 (128-181) months and from first ICD Implantation to the GR was 84 (61-102) months. During a median follow-up of 57 (38-102) months after GR, 10 patients (9%) received successful appropriate ICD intervention (1.6%/year). ICD interventions included shock on ventricular fibrillation ( = 8 patients), shock on ventricular tachycardia ( = 1 patient), and antitachycardia pacing on ventricular tachycardia ( = 1 patient). At survival analysis, history of atrial fibrillation (log-rank test; = 0.02), conduction disturbances (log-rank test; < 0.01), S wave in lead I (log-rank test; = 0.01) and first-degree atrioventricular block (log-rank test; = 0.04) were significantly associated with the occurrence of late appropriate ICD intervention. At Cox-regression multivariate analysis, S-wave in lead I was the only independent predictor of late appropriate ICD intervention (HR: 9.17; 95%CI: 1.15-73.07; = 0.03).
The present study indicates that BrS patient receiving a prophylactic ICD may experience late appropriate intervention after GR in a clinically relevant proportion of cases. S-wave in lead I at the time of first clinical evaluation was the only independent predictor of persistent risk of life-threatening arrhythmic events. These findings support the need for GR at the end of service regardless of previous appropriate intervention, mostly in BrS patients with conduction abnormalities.
对于接受预防性植入式心脏复律除颤器(ICD)的 Brugada 综合征(BrS)患者,危及生命的晚期心律失常事件的预测因素仍有待评估。本长期多中心研究的目的是评估接受预防性 ICD 且正在进行发生器更换(GR)的 BrS 患者中危及生命的晚期心律失常事件的发生率及临床心电图预测因素。
研究人群包括 105 例患者(75%为男性;平均年龄 45±14 岁),这些患者接受了预防性 ICD,且在首次 GR 之前未发生心律失常事件。
从首次 ICD 植入到最后一次随访的中位时间为 155(128 - 181)个月,从首次 ICD 植入到 GR 的时间为 84(61 - 102)个月。在 GR 后的中位随访 57(38 - 102)个月期间,10 例患者(9%)接受了成功的 ICD 恰当干预(1.6%/年)。ICD 干预包括对室颤进行电击(n = 8 例患者)、对室性心动过速进行电击(n = 1 例患者)以及对室性心动过速进行抗心动过速起搏(n = 1 例患者)。在生存分析中,房颤病史(对数秩检验;P = 0.02)、传导障碍(对数秩检验;P < 0.01)、I 导联 S 波(对数秩检验;P = 0.01)和一度房室传导阻滞(对数秩检验;P = 0.04)与晚期 ICD 恰当干预的发生显著相关。在 Cox 回归多变量分析中,I 导联 S 波是晚期 ICD 恰当干预的唯一独立预测因素(HR:9.17;95%CI:1.15 - 73.07;P = 0.03)。
本研究表明,接受预防性 ICD 的 BrS 患者在 GR 后可能会在临床上有意义的比例的病例中经历晚期恰当干预。首次临床评估时 I 导联的 S 波是危及生命的心律失常事件持续风险的唯一独立预测因素。这些发现支持在设备使用期限结束时进行 GR 的必要性,无论之前是否有恰当干预,这主要适用于有传导异常的 BrS 患者。