Xu Yujian, Chen Youbai, Niu Zehao, Yang Zheng, Xing Jiahua, Yin Xiangye, Guo Lingli, Zhang Qixu, Yang Yi, Han Yan
Department of Plastic and Reconstructive Surgery, Chinese PLA General Hospital, Beijing, China.
Department of Plastic Surgery, The University of Texas MD Anderson Cancer Center, Houston, TX, United States.
Front Surg. 2022 Jul 21;9:860806. doi: 10.3389/fsurg.2022.860806. eCollection 2022.
Ferroptosis-related lncRNAs are promising biomarkers for predicting the prognosis of many cancers. However, a ferroptosis-related signature to predict the prognosis of cutaneous melanoma (CM) has not been identified. The purpose of this study was to construct a ferroptosis-related lncRNA signature to predict prognosis and immunotherapy efficacy in CM.
Ferroptosis-related differentially expressed genes (FDEGs) and lncRNAs (FDELs) were identified using TCGA, GTEx, and FerrDb datasets. We performed Cox and LASSO regressions to identify key FDELs, and constructed a risk score to stratify patients into high- and low-risk groups. The lncRNA signature was evaluated using the areas under the receiver operating characteristic curves (AUCs) and Kaplan-Meier analyses in the training, testing, and entire cohorts. Multivariate Cox regression analyses including the lncRNA signature and common clinicopathological characteristics were performed to identify independent predictors of overall survival (OS). A nomogram was developed for clinical use. We performed gene set enrichment analyses (GSEA) to identify significantly enriched pathways. Differences in the tumor microenvironment (TME) between the 2 groups were assessed using 7 algorithms. To predict the efficacy of immune checkpoint inhibitors (ICI), we analyzed the association between and expression and the risk score. Finally, differences in Tumor Mutational Burden (TMB) and molecular drugs Sensitivity between the 2 groups were performed.
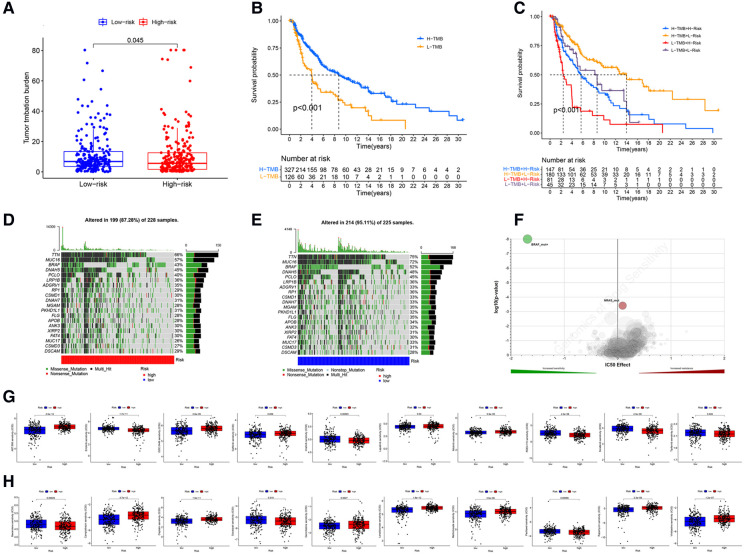
We identified 5 lncRNAs (AATBC, AC145423.2, LINC01871, AC125807.2, and AC245041.1) to construct the risk score. The AUC of the lncRNA signature was 0.743 in the training cohort and was validated in the testing and entire cohorts. Kaplan-Meier analyses revealed that the high-risk group had poorer prognosis. Multivariate Cox regression showed that the lncRNA signature was an independent predictor of OS with higher accuracy than traditional clinicopathological features. The 1-, 3-, and 5-year survival probabilities for CM patients were 92.7%, 57.2%, and 40.2% with an AUC of 0.804, indicating a good accuracy and reliability of the nomogram. GSEA showed that the high-risk group had lower ferroptosis and immune response. TME analyses confirmed that the high-risk group had lower immune cell infiltration (e.g., CD8+ T cells, CD4+ memory-activated T cells, and M1 macrophages) and lower immune functions (e.g., immune checkpoint activation). Low-risk patients whose disease expressed or were likely to respond better to ICIs. The analysis demonstrated that the TMB had significantly difference between low- and high- risk groups. Chemotherapy drugs, such as sorafenib, Imatinib, ABT.888 (Veliparib), Docetaxel, and Paclitaxel showed Significant differences in the estimated IC50 between the two risk groups.
Our novel ferroptosis-related lncRNA signature was able to accurately predict the prognosis and ICI outcomes of CM patients. These ferroptosis-related lncRNAs might be potential biomarkers and therapeutic targets for CM.
铁死亡相关长链非编码RNA(lncRNA)是预测多种癌症预后的有前景的生物标志物。然而,尚未鉴定出用于预测皮肤黑色素瘤(CM)预后的铁死亡相关特征。本研究的目的是构建一种铁死亡相关lncRNA特征,以预测CM的预后和免疫治疗疗效。
使用TCGA、GTEx和FerrDb数据集鉴定铁死亡相关差异表达基因(FDEG)和lncRNA(FDEL)。我们进行了Cox和LASSO回归以鉴定关键FDEL,并构建风险评分以将患者分为高风险和低风险组。在训练、测试和整个队列中,使用受试者工作特征曲线下面积(AUC)和Kaplan-Meier分析评估lncRNA特征。进行多变量Cox回归分析,包括lncRNA特征和常见临床病理特征,以鉴定总生存期(OS)的独立预测因子。开发了用于临床使用的列线图。我们进行基因集富集分析(GSEA)以鉴定显著富集的通路。使用7种算法评估两组之间肿瘤微环境(TME)的差异。为了预测免疫检查点抑制剂(ICI)的疗效,我们分析了 与 表达和风险评分之间的关联。最后,进行两组之间肿瘤突变负荷(TMB)和分子药物敏感性的差异分析。
我们鉴定出5种lncRNA(AATBC、AC145423.2、LINC01871、AC125807.2和AC245041.1)来构建风险评分。lncRNA特征在训练队列中的AUC为0.743,并在测试和整个队列中得到验证。Kaplan-Meier分析显示高风险组预后较差。多变量Cox回归表明,lncRNA特征是OS的独立预测因子,其准确性高于传统临床病理特征。CM患者1年、3年和5年生存概率分别为92.7%、57.2%和40.2%,AUC为0.804,表明列线图具有良好的准确性和可靠性。GSEA显示高风险组铁死亡和免疫反应较低。TME分析证实高风险组免疫细胞浸润较低(如CD8 + T细胞、CD4 + 记忆激活T细胞和M1巨噬细胞)且免疫功能较低(如免疫检查点激活)。疾病表达 或 的低风险患者可能对ICI反应更好。分析表明,低风险和高风险组之间TMB有显著差异。化疗药物,如索拉非尼、伊马替尼、ABT.888(维利帕尼)、多西他赛和紫杉醇在两个风险组之间估计的IC50有显著差异。
我们新的铁死亡相关lncRNA特征能够准确预测CM患者的预后和ICI结果。这些铁死亡相关lncRNA可能是CM的潜在生物标志物和治疗靶点。