School of Medical and Health Sciences, Bangor University, Bangor, UK
School of Medical and Health Sciences, Bangor University, Bangor, UK.
BMJ Open. 2022 Aug 8;12(8):e062392. doi: 10.1136/bmjopen-2022-062392.
To determine intervention effects and synthesise qualitative research that explored women with or at high risk of kidney disease experiences of shared decision-making in relation to their reproductive health, family planning options and pregnancy.
A systematic review of interventions and a qualitative evidence synthesis.
We searched Cochrane, CINAHL, MEDLINE, Scopus, ProQuest, Elsevier, PubMed, ScienceDirect and Web of Science.
Shared decision-making interventions and qualitative studies related to reproductive health involving women with or at high risk of kidney disease published from 1980 until January 2021 in English (clinical settings, global perspective).
Titles were screened against the inclusion criteria and full-text articles were reviewed by the whole team. Framework synthesis was undertaken.
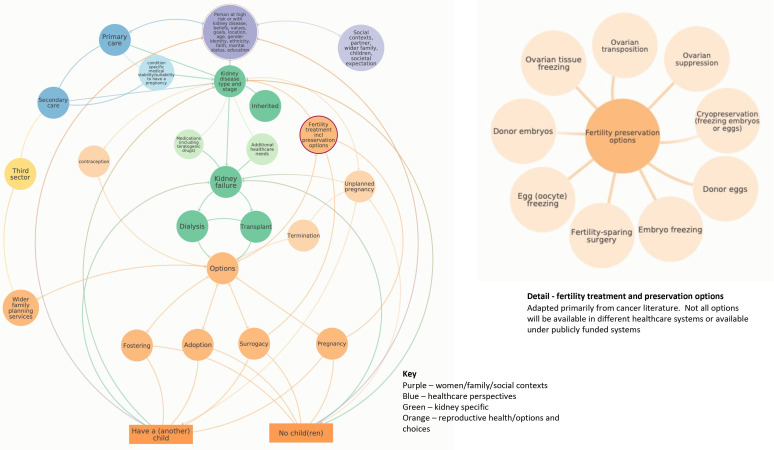
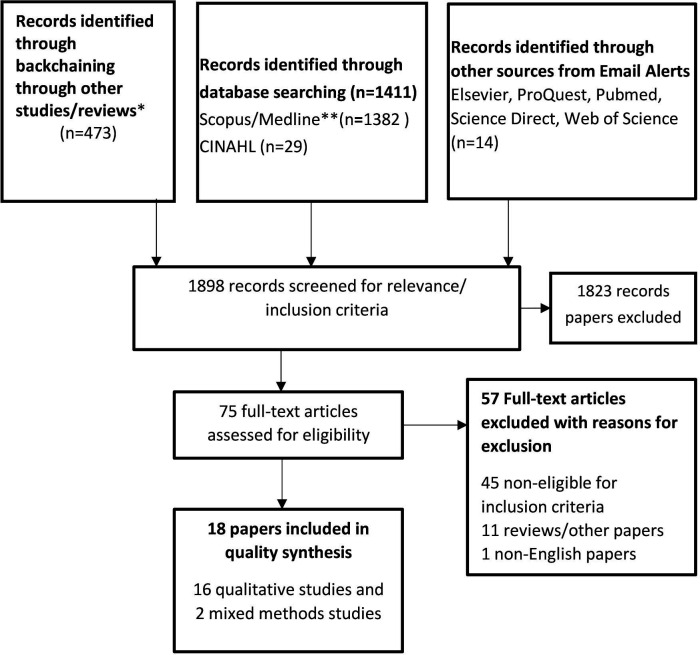
We screened 1898 studies. No evidence-based interventions were identified. 18 qualitative studies were included, 11 kidney disease-specific studies and 7 where kidney disease was a common comorbidity. Women frequently felt unprepared and uninformed about their reproductive options. Conversations with healthcare professionals were commonly described as frustrating and unhelpful, often due to a perceived loss of autonomy and a mismatch in preferences and life goals. Examples of shared decision-making were rare. Kidney disease exacerbated societal expectations of traditional gender roles (eg, wife, mother, carer) including capability to have children and associated factors, for example, parenting, (sexual) relationships, body image and independent living (including financial barriers to starting a family). Local interventions were limited to types of counselling. A new health system model was developed to support new interventions.
There is a clear need to establish new interventions, test those already in development and develop new clinical guidance for the management of women with or at high risk of kidney disease in relation to their reproductive health, including options to preserve fertility earlier. Other health conditions with established personalised reproductive care packages, for example, cancer, could be used to benchmark kidney practice alongside the new model developed here.
确定干预效果,并综合分析探讨患有或有患肾病风险的女性在其生殖健康、计划生育选择和怀孕方面的共享决策体验的定性研究。
干预措施的系统评价和定性证据综合分析。
我们检索了 Cochrane、CINAHL、MEDLINE、Scopus、ProQuest、Elsevier、PubMed、ScienceDirect 和 Web of Science。
1980 年至 2021 年 1 月期间发表的与生殖健康相关的、以英语进行的、针对患有或有患肾病风险的女性的共享决策干预措施和定性研究(临床环境,全球视角)。
对标题进行筛选,以确定是否符合纳入标准,并由全体团队对全文进行了审查。进行了框架综合分析。
我们筛选了 1898 项研究。未发现基于证据的干预措施。共纳入了 18 项定性研究,其中 11 项是针对肾病的具体研究,7 项是肾病常见合并症的研究。女性经常感到对生殖选择毫无准备和不知情。与医疗保健专业人员的沟通通常被描述为令人沮丧和无益,这主要是由于自主权的丧失以及偏好和生活目标的不匹配。共享决策的例子很少见。肾病加剧了社会对传统性别角色的期望(例如,妻子、母亲、照顾者),包括生育能力和相关因素,例如育儿、(性)关系、身体形象和独立生活(包括组建家庭的经济障碍)。当地的干预措施仅限于咨询类型。为支持新的干预措施,开发了一种新的卫生系统模型。
显然需要建立新的干预措施,测试已经在开发中的干预措施,并制定新的临床指南,以管理患有或有患肾病风险的女性的生殖健康,包括更早保留生育能力的选择。其他有既定个性化生殖保健套餐的健康状况,例如癌症,可以与这里开发的新模式一起作为肾病实践的基准。