Kaiser Bonnie N, Gurung Dristy, Rai Sauharda, Bhardwaj Anvita, Dhakal Manoj, Cafaro Cori L, Sikkema Kathleen J, Lund Crick, Patel Vikram, Jordans Mark J D, Luitel Nagendra P, Kohrt Brandon A
University of California San Diego, La Jolla, CA, USA.
Duke Global Health Institute, Durham, NC, USA.
Int J Ment Health Syst. 2022 Aug 11;16(1):37. doi: 10.1186/s13033-022-00546-7.
There are increasing initiatives to reduce mental illness stigma among primary care providers (PCPs) being trained in mental health services. However, there is a gap in understanding how stigma reduction initiatives for PCPs produce changes in attitudes and clinical practices. We conducted a pilot randomized controlled trial of a stigma reduction intervention in Nepal: REducing Stigma among HealthcAre Providers (RESHAPE). In a previous analysis of this pilot, we described differences in stigmatizing attitudes and clinical behaviors between PCPs receiving a standard mental health training (mental health Gap Action Program, mhGAP) vs. those receiving an mhGAP plus RESHAPE training. The goal of this analysis is to use qualitative interview data to explain the quantitative differences in stigma outcomes identified between the trial arms.
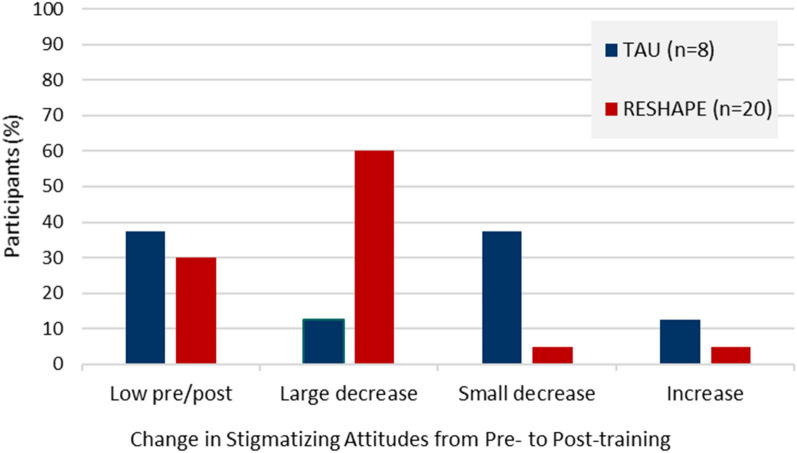
PCPs were randomized to either standard mental health training using mhGAP led by mental health specialists or the experimental condition (RESHAPE) in which service users living with mental illness shared photographic recovery narratives and participated in facilitated social contact. Qualitative interviews were conducted with PCPs five months post-training (n = 8, standard mhGAP training; n = 20, RESHAPE). Stigmatizing attitudes and clinical practices before and after training were qualitatively explored to identify mechanisms of change.
PCPs in both training arms described changes in knowledge, skills, and confidence in providing mental healthcare. PCPs in both arms described a positive feedback loop, in which discussing mental health with patients encouraged more patients to seek treatment and open up about their illness, which demonstrated for PCPs that mental illness can be treated and boosted their clinical confidence. Importantly, PCPs in the RESHAPE arm were more likely to describe a willingness to treat mental health patients and attributed this in part to social contact with service users during the training.
Our qualitative research identified testable mechanisms of action for stigma reduction and improving clinical behavior: specifically, recovery stories from service users and social engagement led to greater willingness to engage with patients about mental illness, triggering a feedback loop of more positive experiences with patients who benefit from mental healthcare, which further reinforces willingness to deliver mental healthcare. Trial registration ClinicalTrials.gov identifier, NCT02793271.
针对接受心理健康服务培训的初级保健提供者(PCP),减少精神疾病污名化的举措越来越多。然而,对于PCP的污名化减少举措如何改变态度和临床实践,目前尚缺乏了解。我们在尼泊尔开展了一项减少污名化干预措施的试点随机对照试验:减少医疗保健提供者中的污名化(RESHAPE)。在对该试点的先前分析中,我们描述了接受标准心理健康培训(心理健康差距行动计划,mhGAP)的PCP与接受mhGAP加RESHAPE培训的PCP在污名化态度和临床行为上的差异。本分析的目的是利用定性访谈数据来解释试验组之间在污名化结果方面的定量差异。
PCP被随机分为两组,一组接受由心理健康专家主导的使用mhGAP的标准心理健康培训,另一组接受实验条件(RESHAPE),即患有精神疾病的服务使用者分享照片康复故事并参与有引导的社交接触。在培训后五个月对PCP进行定性访谈(n = 8,标准mhGAP培训;n = 20,RESHAPE)。定性探索培训前后的污名化态度和临床实践,以确定变化机制。
两个培训组的PCP都描述了在提供心理保健方面知识、技能和信心的变化。两组的PCP都描述了一个积极的反馈循环,即与患者讨论心理健康鼓励更多患者寻求治疗并坦诚自己的病情,这向PCP表明精神疾病是可以治疗的,并增强了他们的临床信心。重要的是,RESHAPE组的PCP更有可能表示愿意治疗精神健康患者,并将其部分归因于培训期间与服务使用者的社交接触。
我们的定性研究确定了减少污名化和改善临床行为的可测试作用机制:具体而言,服务使用者的康复故事和社交参与导致更愿意与患者谈论精神疾病,引发与受益于心理保健的患者更多积极体验的反馈循环,这进一步强化了提供心理保健的意愿。试验注册ClinicalTrials.gov标识符,NCT02793271。