Bai Jinsong, Deng Chaoqiang, Zheng Qiang, Li Di, Fu Fangqiu, Li Yuan, Zhang Yang, Chen Haiquan
Department of Thoracic Surgery and State Key Laboratory of Genetic Engineering, Fudan University Shanghai Cancer Center, Shanghai, China.
Institute of Thoracic Oncology, Fudan University, Shanghai, China.
Transl Lung Cancer Res. 2022 Jul;11(7):1337-1347. doi: 10.21037/tlcr-22-127.
Complex glandular pattern (CGP) was included as high-grade pattern in the new grading system proposed by The International Association for the Study of Lung Cancer. We aimed to investigate the mutational profile and validate the prognostic significance and proper cut-off value to distinguish the aggressive behavior of CGP.
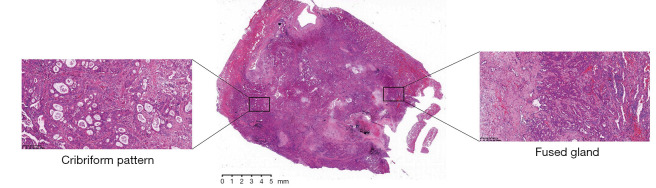
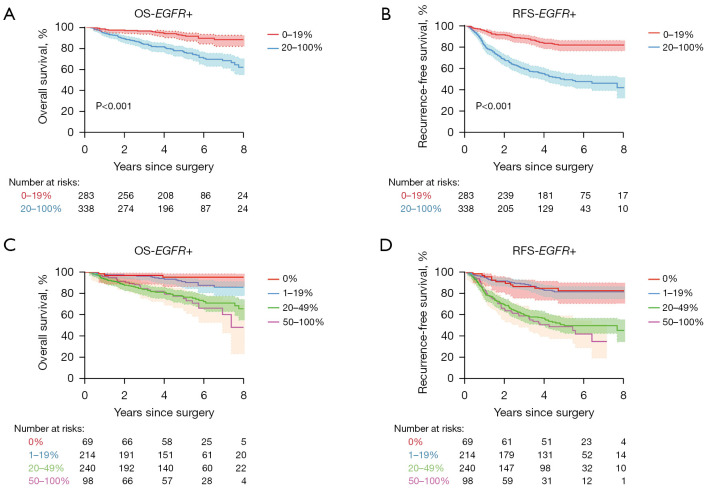
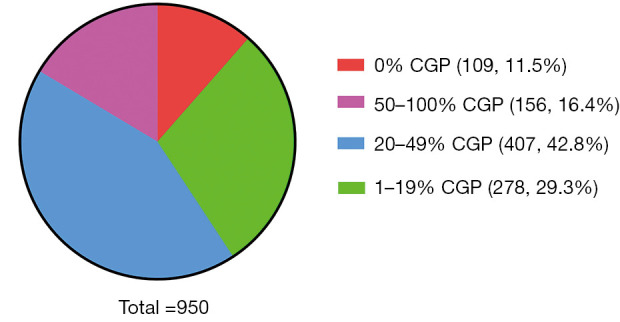
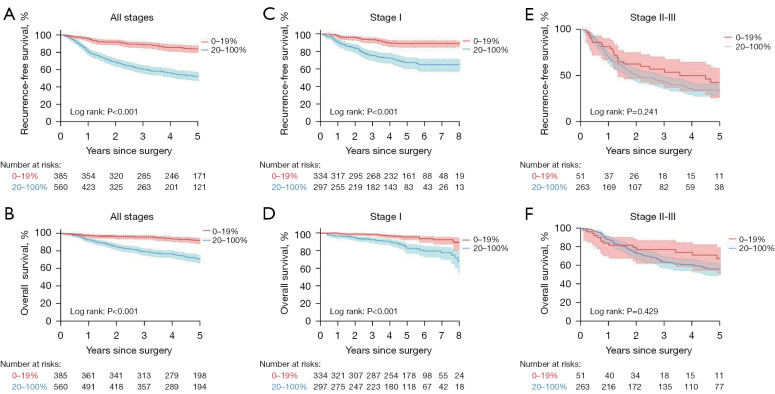
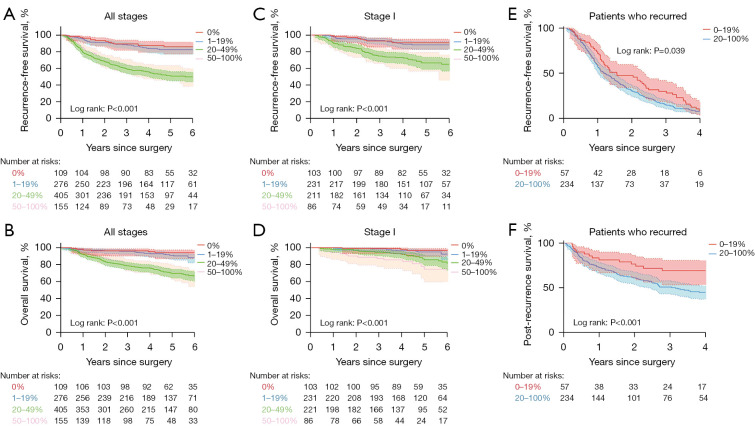
CGP was defined as nests of tumor cells with sieve-like perforation, fused glands with irregular borders or back-to-back glands without intervening stroma. Patients were categorized into four groups according to the percentage of CGP component (0%, 1-19%, 20-49%, 50-100%). Cox's proportional hazards model was applied to analyze recurrence free survival (RFS) and overall survival (OS).
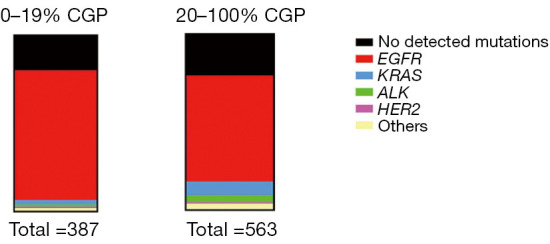
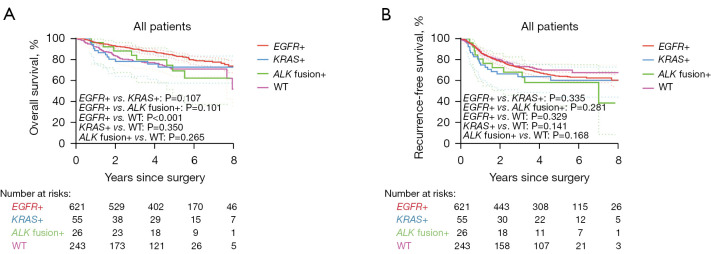
A total of 950 patients with resected lung adenocarcinoma was enrolled. The most frequent driver mutation in this cohort was and was detected in 624 (65.7%) patients. mutation was more frequently observed in patients with <20% CGP than in patients with ≥20% CGP (73.6% 60.2%), while mutation and rearrangement was significantly associated with ≥20% CGP. Patients with 20% or greater CGP exhibited significant worse RFS (P<0.001) and OS (P<0.001) than their counterparts. Moreover, the multivariate Cox regression analysis confirmed that CGP (≥20%) was a risk factor for a worse RFS (P=0.001) and OS (P<0.001) independent of staging and gene mutation. Smaller portion of CGP (<20%) were comparable in RFS and OS to those without CGP (0%). There was also no significant difference in RFS and OS between the 20-49% and ≥50% group.
Our study provided mutational profile of patients with different CGP, validated CGP as a negative prognostic factor and provided extra evidences for the optimal cut-off value of CGP percentage.
复杂腺管模式(CGP)在国际肺癌研究协会提出的新分级系统中被列为高级别模式。我们旨在研究其突变特征,并验证CGP区分侵袭性行为的预后意义及合适的临界值。
CGP定义为具有筛状穿孔的肿瘤细胞巢、边界不规则的融合腺体或无间质间隔的背靠背腺体。根据CGP成分百分比(0%、1 - 19%、20 - 49%、50 - 100%)将患者分为四组。应用Cox比例风险模型分析无复发生存期(RFS)和总生存期(OS)。
共纳入950例接受肺腺癌切除术的患者。该队列中最常见的驱动基因突变是 ,624例(65.7%)患者检测到该突变。CGP < 20%的患者中 突变的观察频率高于CGP≥20%的患者(73.6%对60.2%),而 突变和 重排与CGP≥20%显著相关。CGP≥20%的患者RFS(P < 0.001)和OS(P < 0.001)显著差于CGP < 20%的患者。此外,多因素Cox回归分析证实,CGP(≥20%)是RFS(P = 0.001)和OS(P < 0.001)较差的危险因素,独立于分期和基因突变。CGP比例较小(< 20%)的患者在RFS和OS方面与无CGP(0%)的患者相当。20 - 49%组和≥50%组之间的RFS和OS也无显著差异。
我们的研究提供了不同CGP患者的突变特征,验证了CGP作为不良预后因素,并为CGP百分比的最佳临界值提供了额外证据。