Cramer Holger, Hohmann Christoph, Lauche Romy, Choi Kyung-Eun Anna, Schneider Nadia, Steckhan Nico, Rathjens Florian, Anheyer Dennis, Paul Anna, von Scheidt Christel, Ostermann Thomas, Schneider Elisabeth, Koppold-Liebscher Daniela A, Kessler Christian S, Dobos Gustav, Michalsen Andreas, Jeitler Michael
Department of Internal and Integrative Medicine, Evangelische Kliniken Essen-Mitte, University of Duisburg-Essen, 45276 Essen, Germany.
Institute for General Practice and Interprofessional Care, University Hospital Tuebingen, 72076 Tuebingen, Germany.
J Clin Med. 2022 Aug 14;11(16):4751. doi: 10.3390/jcm11164751.
Lifestyle interventions, such as fasting, diet, and exercise, are increasingly used as a treatment option for patients with metabolic syndrome (MS). This study assesses the efficacy and safety of fasting followed by lifestyle modification in patients with MS compared to lifestyle modification only.
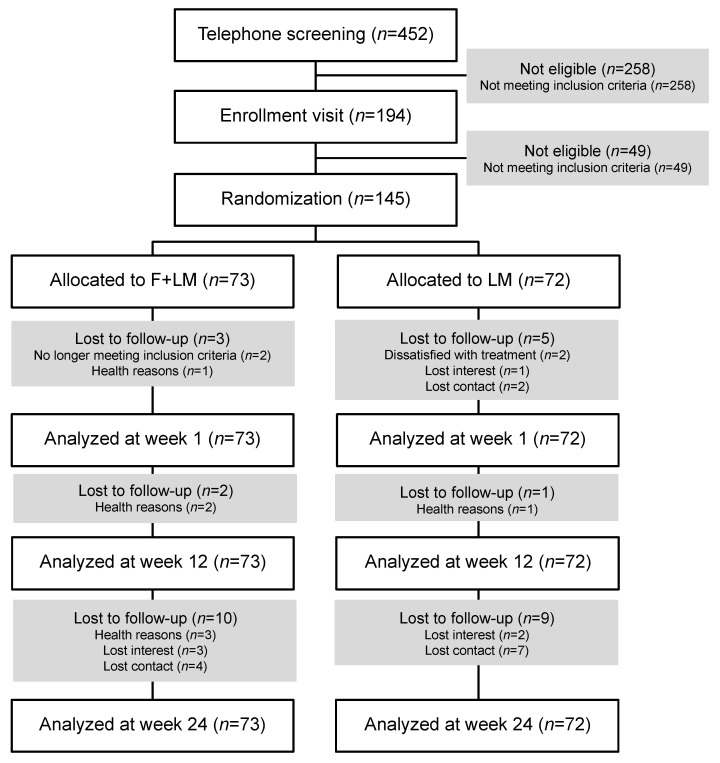
Single-blind, multicenter, parallel, randomized controlled trial in two German tertiary referral hospitals in metropolitan areas.
(a) 5-day fasting followed by 10 weeks of lifestyle modification (modified DASH diet, exercise, mindfulness; = 73); (b) 10 weeks of lifestyle modification only ( = 72).
Co-primary outcomes were ambulatory systolic blood pressure and the homeostasis model assessment (HOMA) index at week 12. Further outcomes included anthropometric, laboratory parameters, and the PROCAM score at weeks 1, 12, and 24.
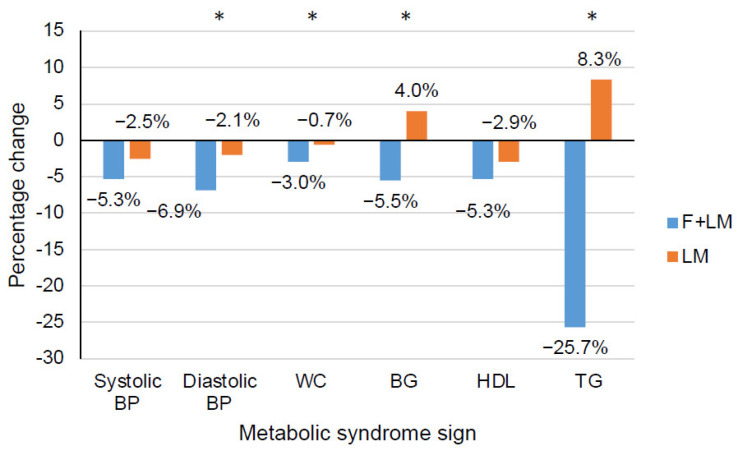
A total of 145 patients with metabolic syndrome (62.8% women; 59.7 ± 9.3 years) were included. No significant group differences occurred for the co-primary outcomes at week 12. However, compared to lifestyle modification only, fasting significantly reduced HOMA index (Δ = -0.8; 95% confidence interval [CI] = -1.7, -0.1), diastolic blood pressure (Δ = -4.8; 95% CI = -5.5, -4.1), BMI (Δ = -1.7; 95% CI = -2.0, -1.4), weight (Δ = -1.7; 95% CI = -2.0, -1.4), waist circumference (Δ = -2.6; 95% CI = -5.0, -0.2), glucose (Δ = -10.3; 95% CI = -19.0, -1.6), insulin (Δ = -2.9; 95% CI = -5.3, -0.4), HbA1c (Δ = -0.2; 95% CI = -0.4, -0.05;), triglycerides (Δ = -48.9; 95% CI = -81.0, -16.9), IL-6 (Δ = -1.2; 95% CI = -2.5, -0.005), and the 10-year risk of acute coronary events (Δ = -4.9; 95% CI = -9.5, -0.4) after week 1. Fasting increased uric acid levels (Δ = 1.0; 95% CI = 0.1, 1.9) and slightly reduced eGRF (Δ = -11.9; 95% CI = -21.8, -2.0). Group differences at week 24 were found for weight (Δ = -2, 7; 95% CI = -4.8, -0.5), BMI (Δ = -1.0; 95% CI = -1.8, -0.3), glucose (Δ = -7.7; 95% CI = -13.5, -1.8), HDL (Δ = 5.1; 95% CI = 1.5, 8.8), and CRP (Δ = 0.2; 95% CI = 0.03, 0.4). No serious adverse events occurred.
A beneficial effect at week 24 was found on weight; fasting also induced various positive short-term effects in patients with MS. Fasting can thus be considered a treatment for initializing lifestyle modification for this patient group; however, it remains to be investigated whether and how the multilayered effects of fasting can be maintained in the medium and longer term.
生活方式干预,如禁食、饮食和运动,越来越多地被用作代谢综合征(MS)患者的一种治疗选择。本研究评估了与仅进行生活方式改变相比,禁食后进行生活方式改变对MS患者的疗效和安全性。
在德国大都市地区的两家三级转诊医院进行单盲、多中心、平行、随机对照试验。
(a)5天禁食,随后进行10周的生活方式改变(改良的得舒饮食、运动、正念;n = 73);(b)仅进行10周的生活方式改变(n = 72)。
共同主要结局是第12周时的动态收缩压和稳态模型评估(HOMA)指数。其他结局包括第1、12和24周时的人体测量、实验室参数和PROCAM评分。
共纳入145例代谢综合征患者(62.8%为女性;59.7±9.3岁)。第12周时共同主要结局无显著组间差异。然而,与仅进行生活方式改变相比,禁食显著降低了HOMA指数(Δ=-0.8;95%置信区间[CI]=-1.7,-0.1)、舒张压(Δ=-4.8;95%CI=-5.5,-4.1)、体重指数(Δ=-1.7;95%CI=-2.0,-1.4)、体重(Δ=-1.7;95%CI=-2.0,-1.4)、腰围(Δ=-2.6;95%CI=-5.0,-0.2)、血糖(Δ=-10.3;95%CI=-19.0,-1.6)、胰岛素(Δ=-2.9;95%CI=-5.3,-0.4)、糖化血红蛋白(Δ=-0.2;95%CI=-0.4,-0.05)、甘油三酯(Δ=-48.9;95%CI=-81.0,-16.9)、白细胞介素-6(Δ=-1.2;95%CI=-2.5,-0.005)以及第1周后急性冠状动脉事件的10年风险(Δ=-4.9;95%CI=-9.5,-0.4)。禁食使尿酸水平升高(Δ=1.0;95%CI=0.1,1.9),并使估算肾小球滤过率略有降低(Δ=-11.9;95%CI=-21.8,-2.0)。第24周时发现组间在体重(Δ=-2.7;95%CI=-4.8,-0.5)、体重指数(Δ=-1.0;95%CI=-1.8,-0.3)、血糖(Δ=-7.7;95%CI=-13.5,-1.8)、高密度脂蛋白(Δ=5.1;95%CI=1.5,8.8)和C反应蛋白(Δ=0.2;95%CI=0.03,0.4)方面存在差异。未发生严重不良事件。
发现第24周时对体重有有益影响;禁食在MS患者中还诱导了各种积极的短期效应。因此,对于该患者群体,禁食可被视为启动生活方式改变的一种治疗方法;然而,禁食的多层效应能否以及如何在中期和长期维持仍有待研究。