Pôle d'Anesthésie-Réanimation, Lille Hospital University, 59000, Lille, France.
Anesthesia and Critical Care Medicine Department, Amiens University Medical Center, 1 rue du Professeur Christian Cabrol, 80054, Amiens, France.
Crit Care. 2022 Aug 26;26(1):257. doi: 10.1186/s13054-022-04133-7.
The mortality rate for a patient with a refractory cardiogenic shock on venoarterial (VA) extracorporeal membrane oxygenation (ECMO) remains high, and hyperoxia might worsen this prognosis. The objective of the present study was to evaluate the association between hyperoxia and 28-day mortality in this setting.
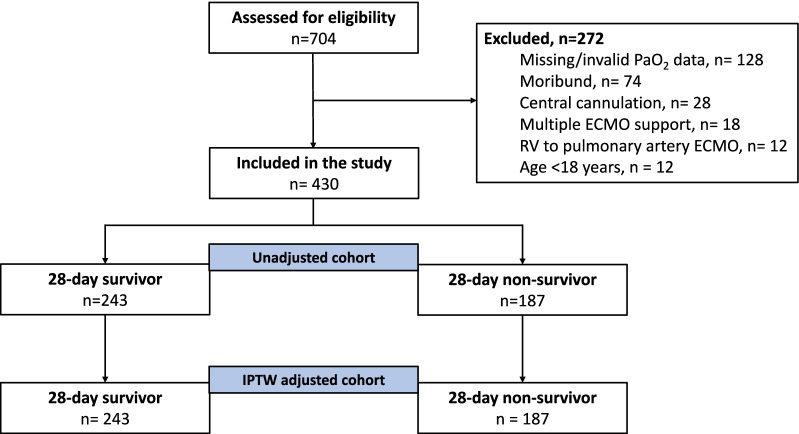
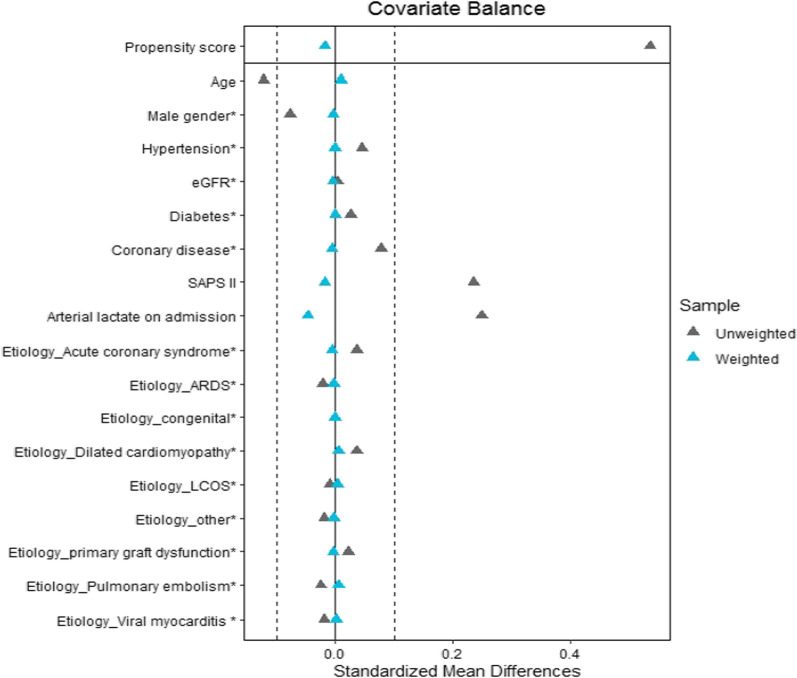
We conducted a retrospective bicenter study in two French academic centers. The study population comprised adult patients admitted for refractory cardiogenic shock. The following arterial partial pressure of oxygen (PaO) variables were recorded for 48 h following admission: the absolute peak PaO (the single highest value measured during the 48 h), the mean daily peak PaO (the mean of each day's peak values), the overall mean PaO (the mean of all values over 48 h), and the severity of hyperoxia (mild: PaO < 200 mmHg, moderate: PaO = 200-299 mmHg, severe: PaO ≥ 300 mmHg). The main outcome was the 28-day all-cause mortality. Inverse probability weighting (IPW) derived from propensity scores was used to reduce imbalances in baseline characteristics.
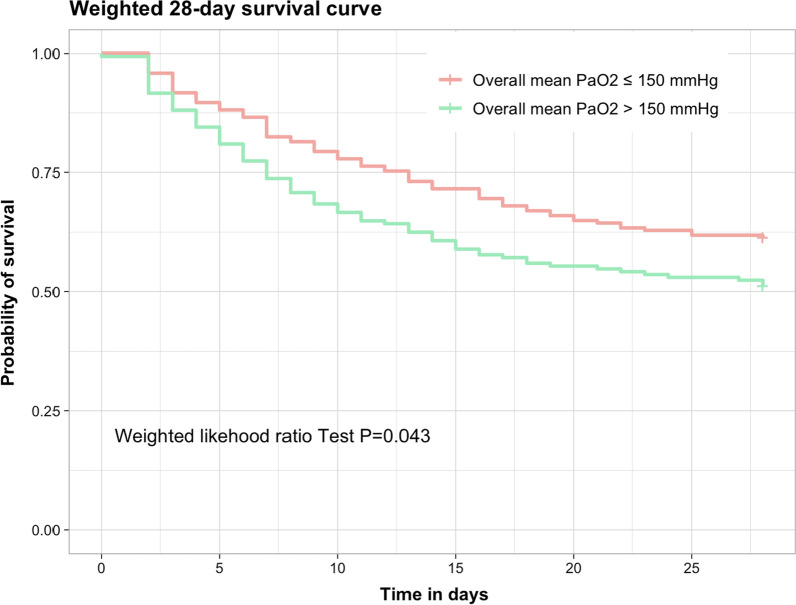
From January 2013 to January 2020, 430 patients were included and assessed. The 28-day mortality rate was 43%. The mean daily peak, absolute peak, and overall mean PaO values were significantly higher in non-survivors than in survivors. In a multivariate logistic regression analysis, the mean daily peak PaO, absolute peak PaO, and overall mean PaO were independent predictors of 28-day mortality (adjusted odds ratio [95% confidence interval per 10 mmHg increment: 2.65 [1.79-6.07], 2.36 [1.67-4.82], and 2.85 [1.12-7.37], respectively). After IPW, high level of oxygen remained significantly associated with 28-day mortality (OR = 1.41 [1.01-2.08]; P = 0.041).
High oxygen levels were associated with 28-day mortality in patients on VA-ECMO support for refractory cardiogenic shock. Our results confirm the need for large randomized controlled trials on this topic.
在接受静脉-动脉体外膜肺氧合(VA-ECMO)治疗的难治性心源性休克患者中,死亡率仍然很高,而高氧可能会使预后恶化。本研究的目的是评估在此情况下高氧与 28 天死亡率之间的关系。
我们在法国的两个学术中心进行了回顾性的双中心研究。研究人群包括因难治性心源性休克而入院的成年患者。在入院后 48 小时内记录以下动脉部分氧分压(PaO)变量:绝对峰值 PaO(48 小时内测量的最高值)、平均每日峰值 PaO(每天峰值的平均值)、总体平均 PaO(48 小时内所有值的平均值)和高氧的严重程度(轻度:PaO<200mmHg,中度:PaO=200-299mmHg,重度:PaO≥300mmHg)。主要结局为 28 天全因死亡率。采用倾向评分逆概率加权(IPW)来减少基线特征的不平衡。
从 2013 年 1 月至 2020 年 1 月,共纳入 430 例患者进行评估。28 天死亡率为 43%。非幸存者的平均每日峰值、绝对峰值和总体平均 PaO 值明显高于幸存者。在多变量逻辑回归分析中,平均每日峰值 PaO、绝对峰值 PaO 和总体平均 PaO 是 28 天死亡率的独立预测因素(每增加 10mmHg 的调整后优势比[95%置信区间]:2.65[1.79-6.07]、2.36[1.67-4.82]和 2.85[1.12-7.37])。在 IPW 后,高水平的氧气仍然与 28 天死亡率显著相关(OR=1.41[1.01-2.08];P=0.041)。
在接受 VA-ECMO 支持治疗难治性心源性休克的患者中,高氧水平与 28 天死亡率相关。我们的结果证实了对此主题进行大型随机对照试验的必要性。