Department of Intensive Care Medicine, Laboratory for Critical Care Computational Intelligence (LCCCI), Amsterdam Medical Data Science (AMDS), Amsterdam Cardiovascular Science (ACS), Amsterdam Institute for Infection and Immunity (AI&II), Amsterdam UMC, Vrije Universiteit, Amsterdam, The Netherlands.
Department of Pharmacy and Clinical Pharmacology, Amsterdam UMC, University of Amsterdam, Amsterdam, The Netherlands.
Crit Care. 2022 Sep 5;26(1):265. doi: 10.1186/s13054-022-04098-7.
Adequate antibiotic dosing may improve outcomes in critically ill patients but is challenging due to altered and variable pharmacokinetics. To address this challenge, AutoKinetics was developed, a decision support system for bedside, real-time, data-driven and personalised antibiotic dosing. This study evaluates the feasibility, safety and efficacy of its clinical implementation.
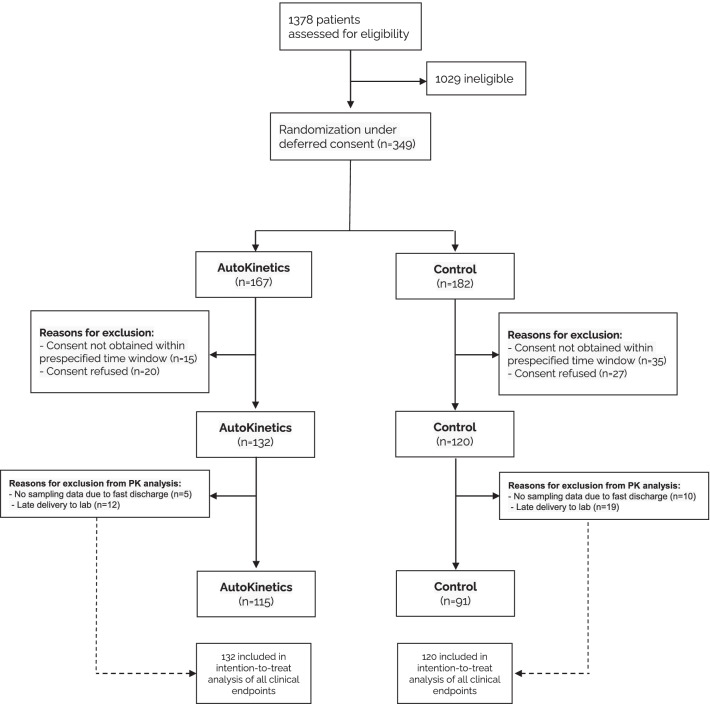
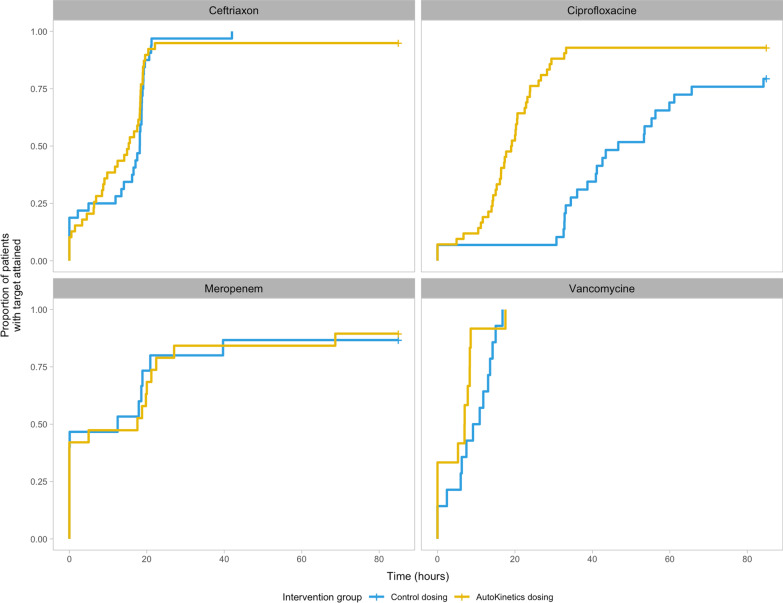
In this two-centre randomised clinical trial, critically ill patients with sepsis or septic shock were randomised to AutoKinetics dosing or standard dosing for four antibiotics: vancomycin, ciprofloxacin, meropenem, and ceftriaxone. Adult patients with a confirmed or suspected infection and either lactate > 2 mmol/L or vasopressor requirement were eligible for inclusion. The primary outcome was pharmacokinetic target attainment in the first 24 h after randomisation. Clinical endpoints included mortality, ICU length of stay and incidence of acute kidney injury.
After inclusion of 252 patients, the study was stopped early due to the COVID-19 pandemic. In the ciprofloxacin intervention group, the primary outcome was obtained in 69% compared to 3% in the control group (OR 62.5, CI 11.4-1173.78, p < 0.001). Furthermore, target attainment was faster (26 h, CI 18-42 h, p < 0.001) and better (65% increase, CI 49-84%, p < 0.001). For the other antibiotics, AutoKinetics dosing did not improve target attainment. Clinical endpoints were not significantly different. Importantly, higher dosing did not lead to increased mortality or renal failure.
In critically ill patients, personalised dosing was feasible, safe and significantly improved target attainment for ciprofloxacin.
The trial was prospectively registered at Netherlands Trial Register (NTR), NL6501/NTR6689 on 25 August 2017 and at the European Clinical Trials Database (EudraCT), 2017-002478-37 on 6 November 2017.
在危重病患者中,适当的抗生素剂量可能会改善治疗效果,但由于药代动力学的改变和变化,这具有一定挑战性。为了解决这一挑战,开发了 AutoKinetics,这是一种床边实时数据驱动和个性化抗生素剂量的决策支持系统。本研究评估了其临床实施的可行性、安全性和疗效。
在这项两中心随机临床试验中,将脓毒症或感染性休克的危重病患者随机分配到 AutoKinetics 剂量组或四种抗生素的标准剂量组:万古霉素、环丙沙星、美罗培南和头孢曲松。纳入标准为乳酸盐>2mmol/L 或需要血管加压药的确诊或疑似感染的成年患者。主要结局是随机分组后 24 小时内的药代动力学目标达标率。临床终点包括死亡率、ICU 住院时间和急性肾损伤的发生率。
纳入 252 例患者后,由于 COVID-19 大流行,研究提前终止。在环丙沙星干预组,主要结局在 69%的患者中达到,而对照组为 3%(OR 62.5,95%CI 11.4-1173.78,p<0.001)。此外,目标达标更快(26 小时,95%CI 18-42 小时,p<0.001)且更好(65%的增加,95%CI 49-84%,p<0.001)。对于其他抗生素,AutoKinetics 剂量并未改善目标达标率。临床终点无显著差异。重要的是,更高的剂量并未导致死亡率或肾衰竭的增加。
在危重病患者中,个性化剂量是可行的、安全的,并显著提高了环丙沙星的目标达标率。
该试验于 2017 年 8 月 25 日在荷兰临床试验注册中心(NTR)前瞻性注册(NTR6501/NTR6689),于 2017 年 11 月 6 日在欧洲临床试验数据库(EudraCT)注册(2017-002478-37)。