Sarraj Mohamed, Hache Philip, Foroutan Farid, Oitment Colby, Marion Travis E, Guha Daipayan, Pahuta Markian
Division of Orthopedic Surgery, Hamilton General Hospital, 3710McMaster University, Hamilton, ON, Canada.
Ted Rogers Centre for Heart Research, 7989University Health Network, Toronto, ON, Canada.
Global Spine J. 2023 Apr;13(3):840-854. doi: 10.1177/21925682221125766. Epub 2022 Sep 7.
Systematic Review.
To conduct a meta-analysis on the survivorship of commonly performed cervical spine procedures to develop survival function curves for (i) second surgery at any cervical level, and (ii) adjacent level surgery.
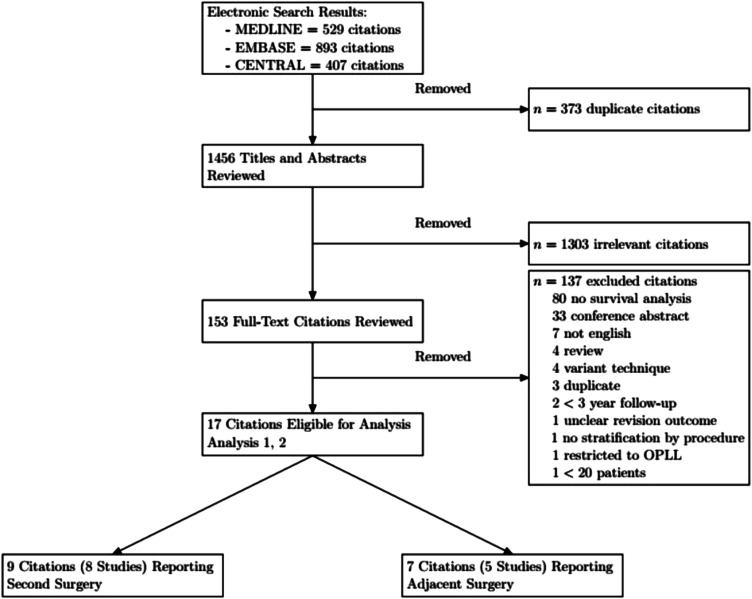
A systematic review of was conducted following PRISMA guidelines. Articles with cohorts of greater than 20 patients followed for a minimum of 36 months and with available survival data were included. Procedures included were anterior cervical discectomy and fusion (ACDF), cervical disc arthroplasty (ADR), laminoplasty (LAMP), and posterior laminectomy and fusion (PDIF). Reconstructed individual patient data were pooled across studies using parametric Bayesian survival meta-regression.
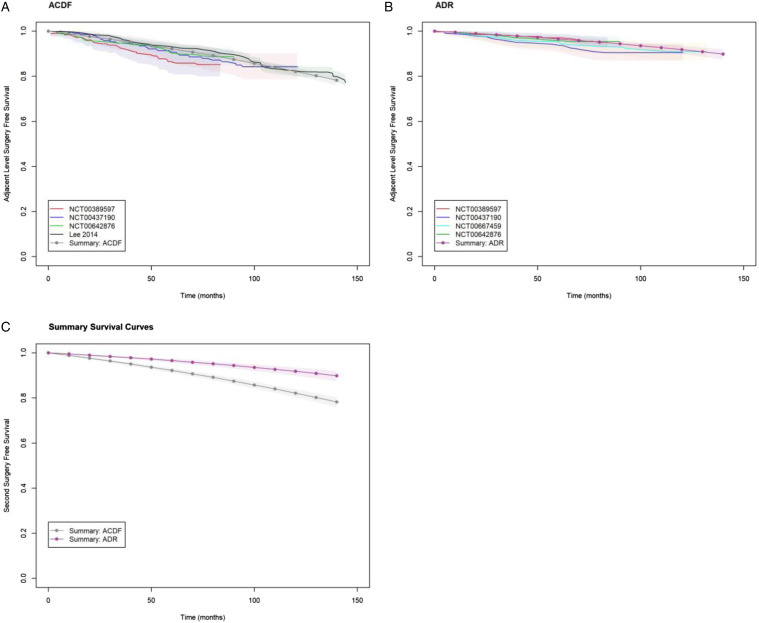
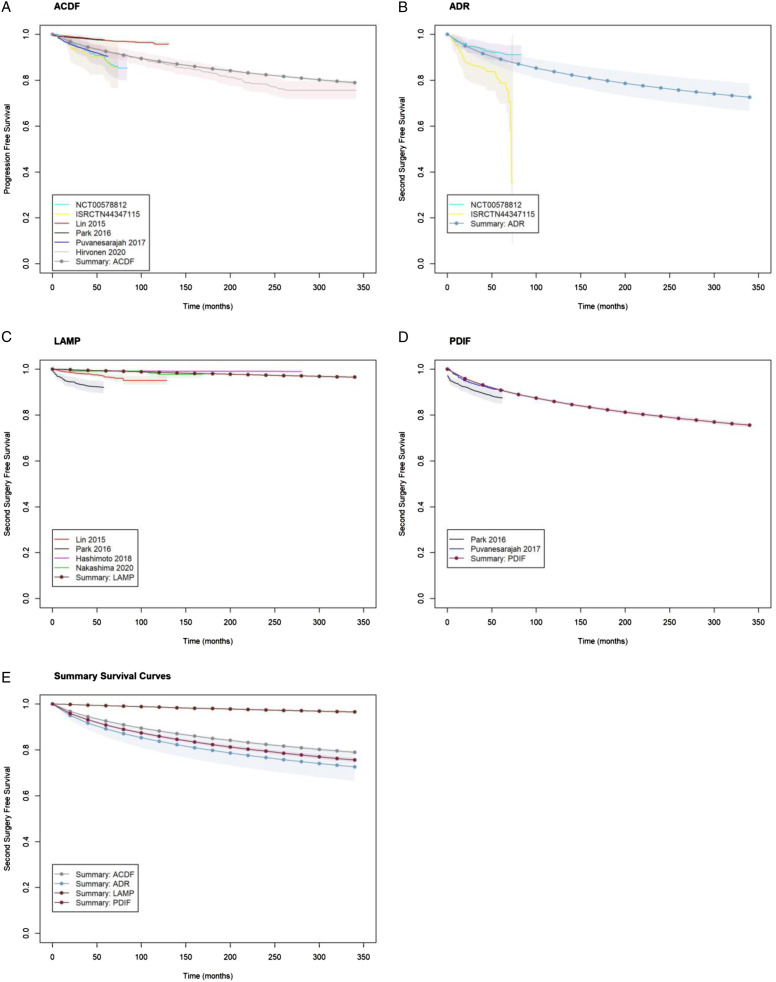
Of 1829 initial titles, 16 citations were included for analysis. 73 811 patients were included in the second surgery analysis and 2858 patients in the adjacent level surgery analysis. We fit a Log normal accelerated failure time model to the second surgery data and a Gompertz proportional hazards model to the adjacent level surgery data. Relative to ACDF, the risk of second surgery was higher with ADR and PDIF with acceleration factors 1.73 (95% CrI: 1.04, 2.80) and 1.35 (95% CrI: 1.25, 1.46) respectively. Relative to ACDF, the risk of second surgery was lower with LAMP with deceleration factor .06 (95% CrI: .05, .07). ADR decreased the risk of adjacent level surgery with hazard ratio .43 (95% CrI: .33, .55).
In cases of clinical equipoise between fusion procedures, our analysis suggests superior survivorship with anterior procedures. For all procedures, laminoplasty demonstrated superior survivorship.
系统评价。
对常见颈椎手术的生存率进行荟萃分析,以绘制(i)颈椎任何节段二次手术和(ii)相邻节段手术的生存功能曲线。
按照PRISMA指南进行系统评价。纳入队列中患者超过20例、随访至少36个月且有可用生存数据的文章。纳入的手术包括颈椎前路椎间盘切除融合术(ACDF)、颈椎间盘置换术(ADR)、椎板成形术(LAMP)以及后路椎板切除融合术(PDIF)。使用参数贝叶斯生存meta回归对各研究中的个体患者重建数据进行汇总。
在1829个初始标题中,纳入16篇文献进行分析。二次手术分析纳入73811例患者,相邻节段手术分析纳入2858例患者。我们对二次手术数据拟合对数正态加速失效时间模型,对相邻节段手术数据拟合Gompertz比例风险模型。相对于ACDF,ADR和PDIF二次手术风险更高,加速因子分别为1.73(95% CrI:1.04,2.80)和1.35(95% CrI:1.25,1.46)。相对于ACDF,LAMP二次手术风险更低,减速因子为0.06(95% CrI:0.05,0.07)。ADR降低相邻节段手术风险,风险比为0.43(95% CrI:0.33,0.55)。
在融合手术之间存在临床 equipoise 的情况下,我们的分析表明前路手术生存率更高。对于所有手术,椎板成形术显示出更高的生存率。