Pahuta Markian, Sarraj Mohamed, Busse Jason, Guha Daipayan, Bhandari Mohit
Division of Orthopedic Surgery, Hamilton General Hospital, McMaster University, Hamilton, Ontario, Canada.
Departments of Anesthesia and Health Evidence and Impact, McMaster University, Hamilton, Ontario, Canada.
JB JS Open Access. 2024 Nov 21;9(4). doi: 10.2106/JBJS.OA.23.00166. eCollection 2024 Oct-Dec.
Degenerative cervical myelopathy (DCM) occurs when spondylotic changes compress the spinal cord and cause neurologic dysfunction. Because of a lack of comparative data on nonoperative care versus surgery for DCM, it has been difficult to support patients through the shared decision-making process regarding treatment options. Our objective was to synthesize the best available data in a manner that helps clinicians and patients to weigh the differences between nonoperative care and surgery at different ages and disease severity. The 2 patient-centered questions we sought to answer were (1) "am I more likely to experience worsening myelopathy with nonoperative care, or need more surgery if I have my myelopathy treated operatively?" and (2) "how much better will my quality of life be with nonoperative care versus surgery?"
We used a health economic technique, microsimulation, to model head-to-head comparisons of nonoperative care versus surgery for DCM. We incorporated the best available data, modeled patients over a lifetime horizon, used direct comparators, and incorporated uncertainty in both natural history and treatment effect.
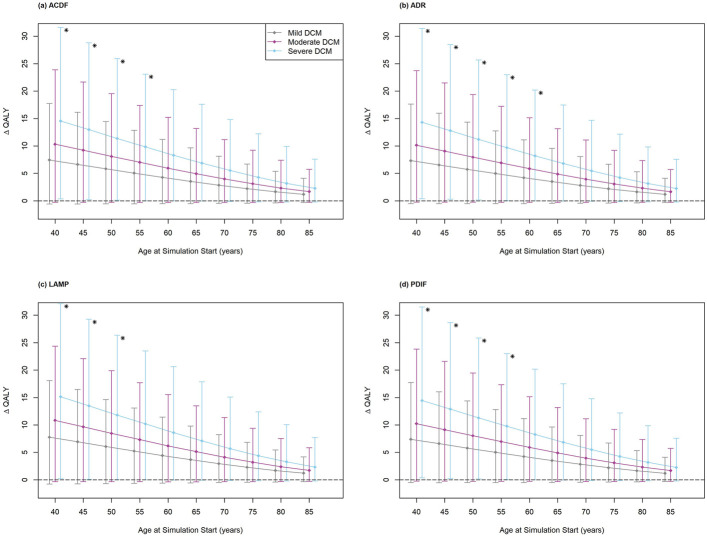
Patients with mild DCM at baseline who were ≥75 years of age were less likely to neurologically decline under nonoperative care than to undergo a second surgery if the index surgery was an anterior cervical discectomy and fusion (ACDF), cervical disc arthroplasty (ADR), or posterior cervical decompression and instrumented fusion (PDIF). Using quality-adjusted life-years (QALYs), our results suggest that surgery for DCM may be superior to nonoperative care. However, for all patients except those with severe DCM who are of middle age or younger (depending on the procedure, ≤50 to ≤60 years of age), the lower bound of the 95% confidence interval for the estimated difference in QALYs was <0.
In most patient groups, neurologic progression with nonoperative management is more likely than the need for additional cervical surgery following operative management, with the exception of patients 75 to 80 years of age and older with mild DCM. Furthermore, on average, surgery for DCM tends to improve quality of life. However, patients with DCM who are older than middle age should be aware that the estimates of the quality-of-life benefit are highly uncertain, with a lower bound of <0.
Therapeutic Level III. See Instructions for Authors for a complete description of levels of evidence.
当脊柱退变改变压迫脊髓并导致神经功能障碍时,会发生退行性颈椎脊髓病(DCM)。由于缺乏关于DCM非手术治疗与手术治疗的比较数据,因此在帮助患者进行关于治疗方案的共同决策过程中一直存在困难。我们的目标是以一种有助于临床医生和患者权衡不同年龄和疾病严重程度下非手术治疗与手术治疗差异的方式,综合现有最佳数据。我们试图回答的两个以患者为中心的问题是:(1)“如果我接受非手术治疗,脊髓病恶化的可能性是否更大,或者如果我接受手术治疗脊髓病,是否需要更多手术?”以及(2)“与手术相比,非手术治疗能使我的生活质量提高多少?”
我们使用一种健康经济技术,即微观模拟,对DCM的非手术治疗与手术治疗进行直接比较建模。我们纳入了现有最佳数据,对患者一生的情况进行建模,使用直接比较对象,并纳入了自然病程和治疗效果方面的不确定性。
基线时患有轻度DCM且年龄≥75岁的患者,如果初次手术是前路颈椎间盘切除融合术(ACDF)、颈椎间盘置换术(ADR)或后路颈椎减压及器械融合术(PDIF),那么在非手术治疗下神经功能衰退的可能性低于接受二次手术的可能性。使用质量调整生命年(QALY),我们的结果表明,DCM手术治疗可能优于非手术治疗。然而,对于所有患者,除了中年或更年轻的重度DCM患者(取决于手术方式,年龄≤50至≤60岁),QALY估计差异的95%置信区间下限<0。
在大多数患者群体中,非手术治疗导致神经功能进展的可能性大于手术治疗后需要额外颈椎手术的可能性,但75至80岁及以上患有轻度DCM的患者除外。此外,平均而言,DCM手术治疗往往能改善生活质量。然而,中年以上的DCM患者应意识到,生活质量获益的估计存在高度不确定性,下限<0。
治疗性III级。有关证据水平的完整描述,请参阅作者指南。