Imagen Technologies, New York, NY, USA.
The Mount Sinai Hospital, New York, NY, USA.
Clin Orthop Relat Res. 2023 Mar 1;481(3):580-588. doi: 10.1097/CORR.0000000000002385. Epub 2022 Sep 9.
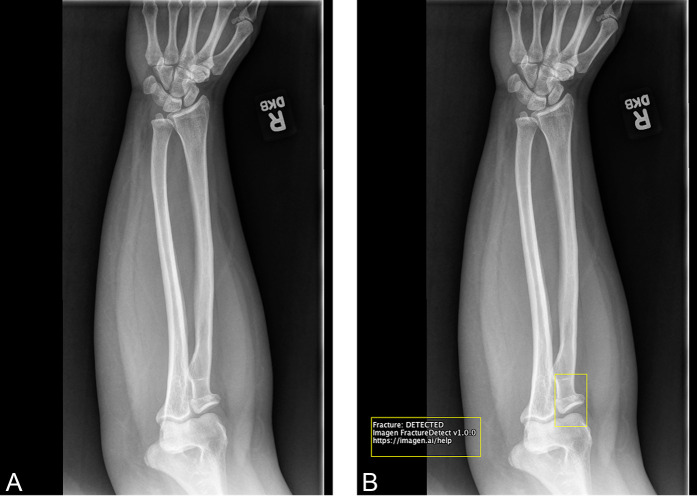
Missed fractures are the most common diagnostic errors in musculoskeletal imaging and can result in treatment delays and preventable morbidity. Deep learning, a subfield of artificial intelligence, can be used to accurately detect fractures by training algorithms to emulate the judgments of expert clinicians. Deep learning systems that detect fractures are often limited to specific anatomic regions and require regulatory approval to be used in practice. Once these hurdles are overcome, deep learning systems have the potential to improve clinician diagnostic accuracy and patient care.
QUESTIONS/PURPOSES: This study aimed to evaluate whether a Food and Drug Administration-cleared deep learning system that identifies fractures in adult musculoskeletal radiographs would improve diagnostic accuracy for fracture detection across different types of clinicians. Specifically, this study asked: (1) What are the trends in musculoskeletal radiograph interpretation by different clinician types in the publicly available Medicare claims data? (2) Does the deep learning system improve clinician accuracy in diagnosing fractures on radiographs and, if so, is there a greater benefit for clinicians with limited training in musculoskeletal imaging?
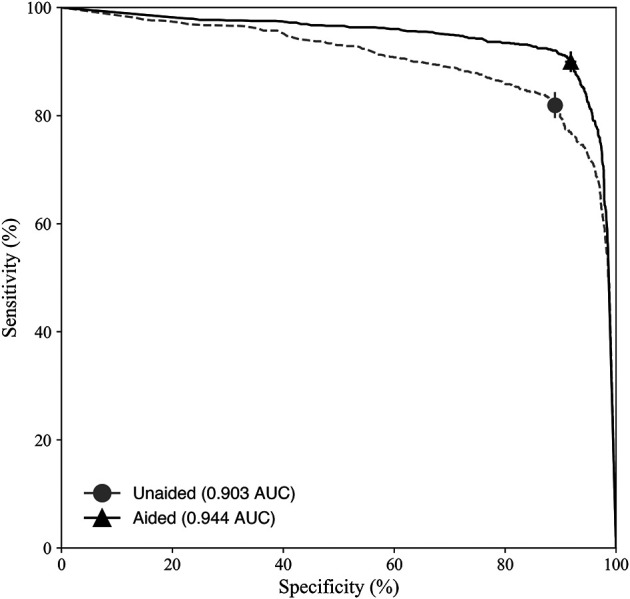
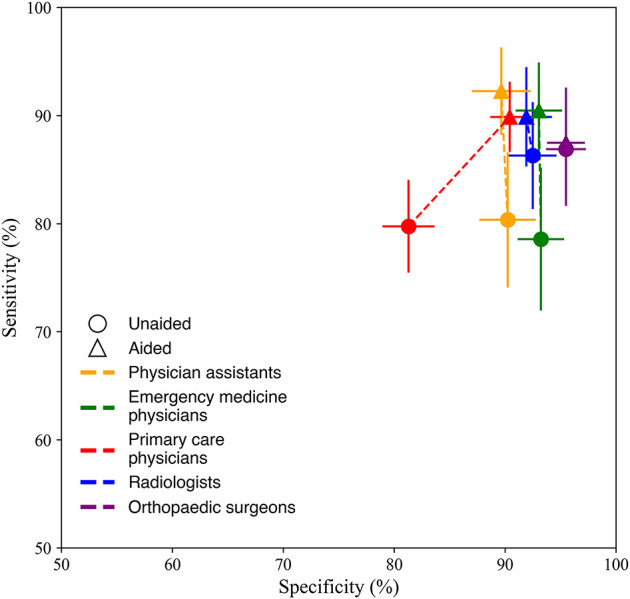
We used the publicly available Medicare Part B Physician/Supplier Procedure Summary data provided by the Centers for Medicare & Medicaid Services to determine the trends in musculoskeletal radiograph interpretation by clinician type. In addition, we conducted a multiple-reader, multiple-case study to assess whether clinician accuracy in diagnosing fractures on radiographs was superior when aided by the deep learning system compared with when unaided. Twenty-four clinicians (radiologists, orthopaedic surgeons, physician assistants, primary care physicians, and emergency medicine physicians) with a median (range) of 16 years (2 to 37) of experience postresidency each assessed 175 unique musculoskeletal radiographic cases under aided and unaided conditions (4200 total case-physician pairs per condition). These cases were comprised of radiographs from 12 different anatomic regions (ankle, clavicle, elbow, femur, forearm, hip, humerus, knee, pelvis, shoulder, tibia and fibula, and wrist) and were randomly selected from 12 hospitals and healthcare centers. The gold standard for fracture diagnosis was the majority opinion of three US board-certified orthopaedic surgeons or radiologists who independently interpreted the case. The clinicians' diagnostic accuracy was determined by the area under the curve (AUC) of the receiver operating characteristic (ROC) curve, sensitivity, and specificity. Secondary analyses evaluated the fracture miss rate (1-sensitivity) by clinicians with and without extensive training in musculoskeletal imaging.
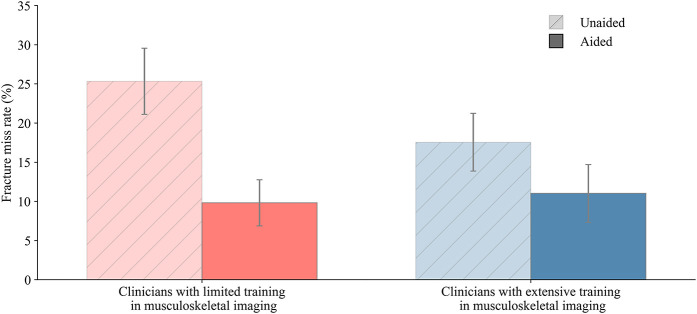
Medicare claims data revealed that physician assistants showed the greatest increase in interpretation of musculoskeletal radiographs within the analyzed time period (2012 to 2018), although clinicians with extensive training in imaging (radiologists and orthopaedic surgeons) still interpreted the majority of the musculoskeletal radiographs. Clinicians aided by the deep learning system had higher accuracy diagnosing fractures in radiographs compared with when unaided (unaided AUC: 0.90 [95% CI 0.89 to 0.92]; aided AUC: 0.94 [95% CI 0.93 to 0.95]; difference in least square mean per the Dorfman, Berbaum, Metz model AUC: 0.04 [95% CI 0.01 to 0.07]; p < 0.01). Clinician sensitivity increased when aided compared with when unaided (aided: 90% [95% CI 88% to 92%]; unaided: 82% [95% CI 79% to 84%]), and specificity increased when aided compared with when unaided (aided: 92% [95% CI 91% to 93%]; unaided: 89% [95% CI 88% to 90%]). Clinicians with limited training in musculoskeletal imaging missed a higher percentage of fractures when unaided compared with radiologists (miss rate for clinicians with limited imaging training: 20% [95% CI 17% to 24%]; miss rate for radiologists: 14% [95% CI 9% to 19%]). However, when assisted by the deep learning system, clinicians with limited training in musculoskeletal imaging reduced their fracture miss rate, resulting in a similar miss rate to radiologists (miss rate for clinicians with limited imaging training: 9% [95% CI 7% to 12%]; miss rate for radiologists: 10% [95% CI 6% to 15%]).
Clinicians were more accurate at diagnosing fractures when aided by the deep learning system, particularly those clinicians with limited training in musculoskeletal image interpretation. Reducing the number of missed fractures may allow for improved patient care and increased patient mobility.
Level III, diagnostic study.
在肌肉骨骼成像中,漏诊骨折是最常见的诊断错误,可能导致治疗延误和可预防的发病率增加。深度学习是人工智能的一个分支,可以通过训练算法来模拟专家临床医生的判断,从而准确地检测骨折。专门用于检测骨折的深度学习系统通常仅限于特定的解剖区域,并且需要监管部门批准才能在实践中使用。一旦克服了这些障碍,深度学习系统有可能提高临床医生的诊断准确性并改善患者护理。
问题/目的:本研究旨在评估一种已获得美国食品和药物管理局批准的深度学习系统,该系统可识别成人肌肉骨骼 X 光片中的骨折,是否可以提高不同类型临床医生检测骨折的准确性。具体而言,本研究提出了以下两个问题:(1)在公开的医疗保险索赔数据中,不同类型的临床医生在肌肉骨骼 X 光片解读方面的趋势是什么?(2)深度学习系统是否可以提高临床医生在 X 光片上诊断骨折的准确性,如果可以,那么在肌肉骨骼成像方面接受有限培训的临床医生是否会获得更大的收益?
我们使用美国医疗保险部分 B 医师/供应商程序摘要数据(由医疗保险和医疗补助服务中心提供)来确定不同类型临床医生解读肌肉骨骼 X 光片的趋势。此外,我们进行了一项多读者、多案例研究,以评估与未辅助时相比,临床医生在辅助深度学习系统时诊断 X 光片骨折的准确性是否更高。24 名临床医生(放射科医生、骨科医生、医师助理、初级保健医生和急诊医生)在住院后具有中位数(范围)为 16 年(2 至 37 年)的经验,每个临床医生评估了 175 个独特的肌肉骨骼放射学案例,分别处于辅助和未辅助条件下(每个条件下每个案例的医生为 4200 对)。这些案例包括来自 12 个不同解剖区域(脚踝、锁骨、肘部、股骨、前臂、臀部、肱骨、膝盖、骨盆、肩部、胫骨和腓骨以及手腕)的 X 光片,并且是从 12 家医院和医疗中心随机选择的。骨折诊断的金标准是三位美国董事会认证的骨科医生或放射科医生的多数意见,他们独立地解读了该病例。临床医生的诊断准确性由接受者操作特征(ROC)曲线的曲线下面积(AUC)、灵敏度和特异性来确定。次要分析评估了有和没有肌肉骨骼成像广泛培训的临床医生的骨折漏诊率(1-灵敏度)。
医疗保险索赔数据显示,在分析期间(2012 年至 2018 年),医师助理在解读肌肉骨骼 X 光片方面的增幅最大,尽管在成像方面接受过广泛培训的临床医生(放射科医生和骨科医生)仍解读了大多数肌肉骨骼 X 光片。与未辅助时相比,临床医生辅助深度学习系统时的骨折诊断准确性更高(未辅助时 AUC:0.90 [95% CI 0.89 至 0.92];辅助时 AUC:0.94 [95% CI 0.93 至 0.95];根据 Dorfman、Berbaum、Metz 模型的最小平方均值差异 AUC:0.04 [95% CI 0.01 至 0.07];p < 0.01)。与未辅助时相比,辅助时临床医生的灵敏度增加(辅助时:90% [95% CI 88% 至 92%];未辅助时:82% [95% CI 79% 至 84%]),特异性也增加(辅助时:92% [95% CI 91% 至 93%];未辅助时:89% [95% CI 88% 至 90%])。在肌肉骨骼成像方面接受有限培训的临床医生未辅助时漏诊骨折的比例更高,与放射科医生相比(接受有限成像培训的临床医生的漏诊率:20% [95% CI 17% 至 24%];放射科医生的漏诊率:14% [95% CI 9% 至 19%])。然而,当临床医生接受深度学习系统辅助时,在肌肉骨骼成像方面接受有限培训的临床医生降低了他们的骨折漏诊率,从而使他们的漏诊率与放射科医生相似(接受有限成像培训的临床医生的漏诊率:9% [95% CI 7% 至 12%];放射科医生的漏诊率:10% [95% CI 6% 至 15%])。
临床医生在辅助深度学习系统时,骨折诊断的准确性更高,特别是在肌肉骨骼图像解读方面接受有限培训的临床医生。减少漏诊骨折的数量可能会提高患者护理水平并增加患者的活动能力。
III 级,诊断研究。