Xu Wenchang, Zhang Fengjun, Shi Yingzhou, Chen Yuanzhen, Shi Bin, Yu Gongchang
School of Acupuncture and Tuina, Shandong University of Traditional Chinese Medicine, Jinan, China.
Neck-Shoulder and Lumbocrural Pain Hospital of Shandong First Medical University, Shandong First Medical University and Shandong Academy of Medical Sciences, Jinan, China.
Front Med (Lausanne). 2022 Sep 23;9:989950. doi: 10.3389/fmed.2022.989950. eCollection 2022.
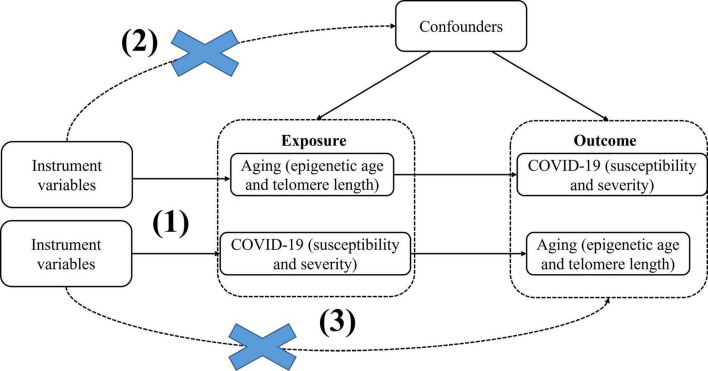
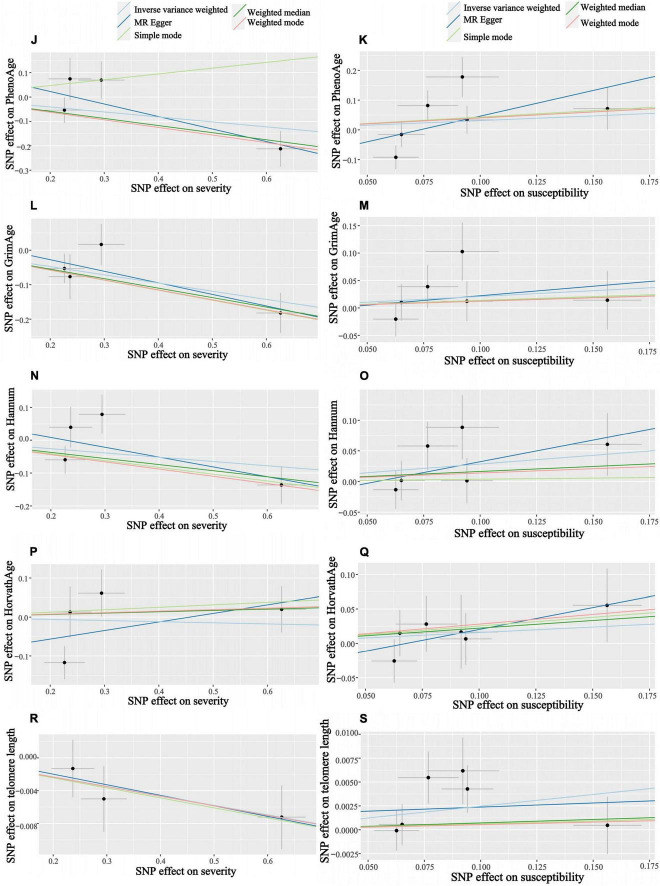
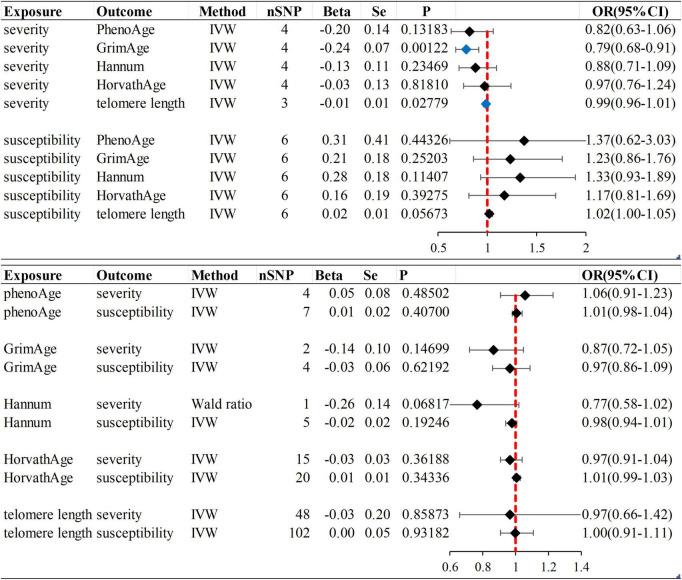
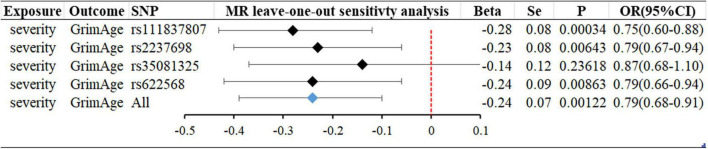
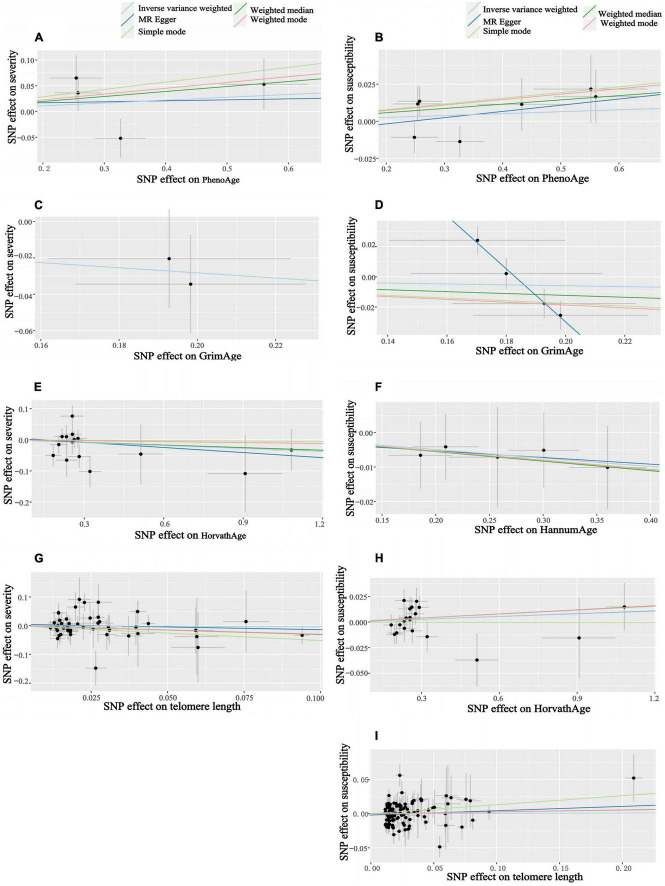
Observational data from China, the United States, France, and Italy suggest that chronological age is an adverse COVID-19 outcome risk factor, with older patients having a higher severity and mortality rate than younger patients. Most studies have gotten the same view. However, the role of aging in COVID-19 adverse effects is unclear. To more accurately assess the effect of aging on adverse COVID-19, we conducted this bidirectional Mendelian randomization (MR) study. Epigenetic clocks and telomere length were used as biological indicators of aging. Data on epigenetic age (PhenoAge, GrimAge, Intrinsic HorvathAge, and HannumAge) were derived from an analysis of biological aging based on genome-wide association studies (GWAS) data. The telomere length data are derived from GWAS and the susceptibility and severity data are derived from the COVID-19 Host Genetics Initiative (HGI). Firstly, epigenetic age and telomere length were used as exposures, and following a screen for appropriate instrumental variables, we used random-effects inverse variance weighting (IVW) for the main analysis, and combined it with other analysis methods (e.g., MR Egger, Weighted median, simple mode, Weighted mode) and multiple sensitivity analysis (heterogeneity analysis, horizontal multiplicity analysis, "leave-one-out" analysis). For reducing false-positive rates, Bonferroni corrected significance thresholds were used. A reverse Mendelian randomization analysis was subsequently performed with COVID-19 susceptibility and severity as the exposure. The results of the MR analysis showed no significant differences in susceptibility to aging and COVID-19. It might suggest that aging is not a risk factor for COVID-19 infection (-values are in the range of 0.05-0.94). According to the results of our analysis, we found that aging was not a risk factor for the increased severity of COVID-19 ( > 0.05). However, severe COVID-19 can cause telomere lengths to become shorter (beta = -0.01; se = 0.01; = 0.02779). In addition to this, severe COVID-19 infection can slow the acceleration of the epigenetic clock "GrimAge" (beta = -0.24, se = 0.07, = 0.00122), which may be related to the closely correlation of rs35081325 and COVID-19 severity. Our study provides partial evidence for the causal effects of aging on the susceptibility and severity of COVID-19.
来自中国、美国、法国和意大利的观察数据表明,实际年龄是新冠病毒疾病不良预后的一个风险因素,老年患者比年轻患者的病情更严重,死亡率更高。大多数研究都得出了相同的观点。然而,衰老在新冠病毒疾病不良影响中的作用尚不清楚。为了更准确地评估衰老对新冠病毒疾病不良影响的作用,我们开展了这项双向孟德尔随机化(MR)研究。表观遗传时钟和端粒长度被用作衰老的生物学指标。表观遗传年龄数据(PhenoAge、GrimAge、内在霍瓦斯年龄和汉努姆年龄)来自基于全基因组关联研究(GWAS)数据的生物衰老分析。端粒长度数据来自GWAS,易感性和严重程度数据来自新冠病毒疾病宿主遗传学倡议(HGI)。首先,将表观遗传年龄和端粒长度用作暴露因素,在筛选出合适的工具变量后,我们使用随机效应逆方差加权法(IVW)进行主要分析,并将其与其他分析方法(如MR Egger、加权中位数、简单模式、加权模式)以及多种敏感性分析(异质性分析、水平多重性分析、“留一法”分析)相结合。为降低假阳性率,使用了Bonferroni校正的显著性阈值。随后进行了反向孟德尔随机化分析,将新冠病毒疾病易感性和严重程度作为暴露因素。MR分析结果显示衰老与新冠病毒疾病易感性之间无显著差异。这可能表明衰老不是新冠病毒感染的风险因素(P值在0.05 - 0.94范围内)。根据我们的分析结果,我们发现衰老不是新冠病毒疾病严重程度增加的风险因素(P > 0.05)。然而,严重的新冠病毒疾病会导致端粒长度缩短(β = -0.01;标准误 = 0.01;P = 0.02779)。除此之外,严重的新冠病毒感染会减缓表观遗传时钟“GrimAge”的加速(β = -0.24,标准误 = 0.07,P = 0.00122),这可能与rs35081325和新冠病毒疾病严重程度密切相关。我们的研究为衰老对新冠病毒疾病易感性和严重程度的因果效应提供了部分证据。