Department of Orthopedic Surgery, Peking University First Hospital, Beijing, China.
Department of Orthopaedic Surgery, Shanghai Sixth People's Hospital Affiliated to Shanghai Jiao Tong University, Shanghai, China.
Front Public Health. 2022 Oct 6;10:1019168. doi: 10.3389/fpubh.2022.1019168. eCollection 2022.
Bone is one of the most common sites for the spread of malignant tumors. Patients with bone metastases whose prognosis was shorter than 3 months (early death) were considered as surgical contraindications. However, the information currently available in the literature limits our capacity to assess the risk likelihood of 3 month mortality. As a result, the study's objective is to create an accurate prediction model utilizing machine-learning techniques to predict 3 month mortality specifically among lung cancer patients with bone metastases according to easily available clinical data.
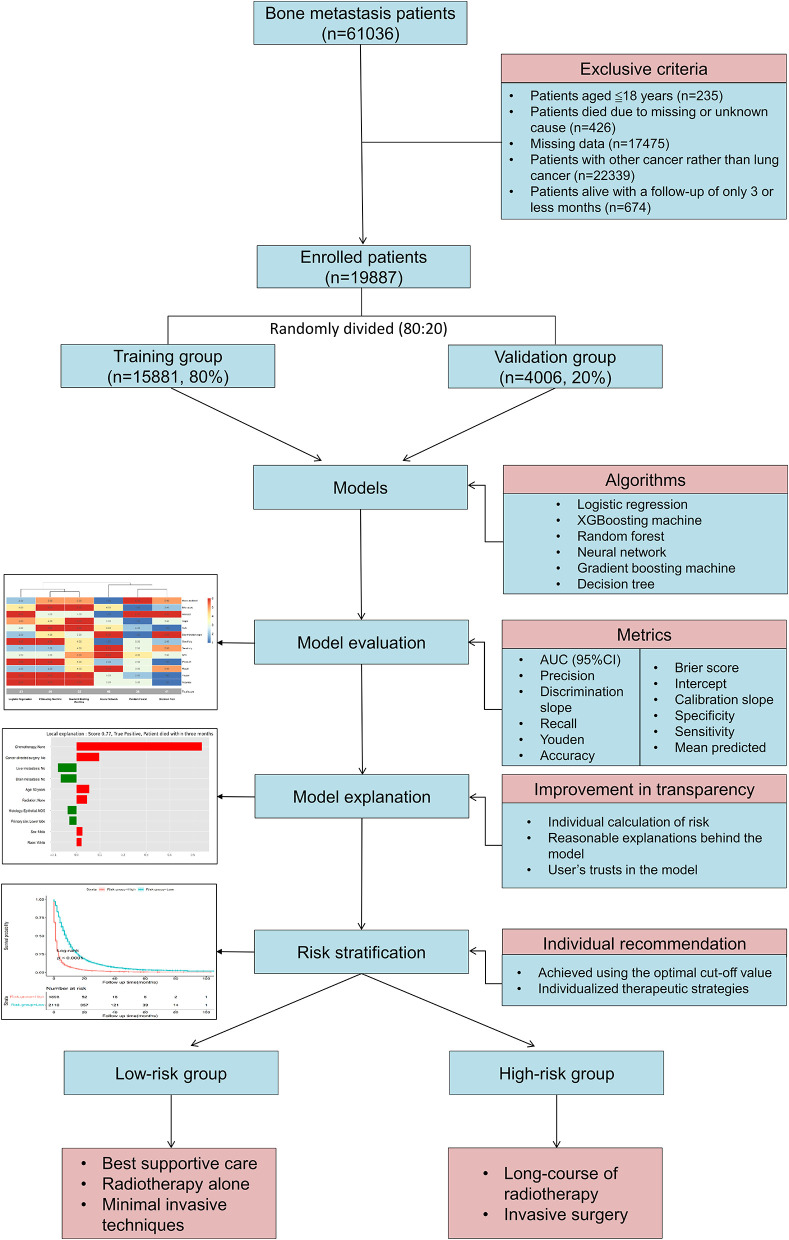
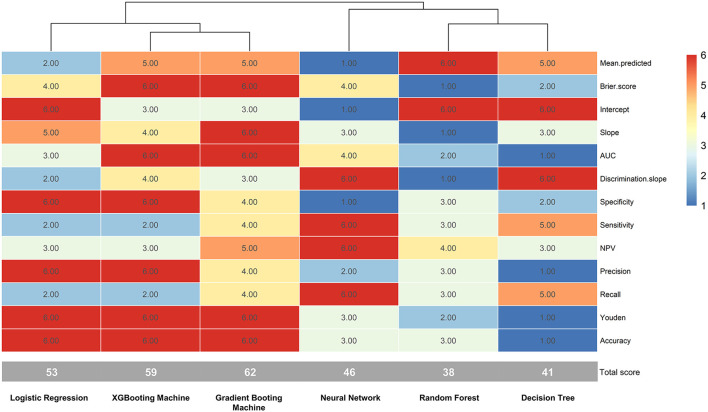
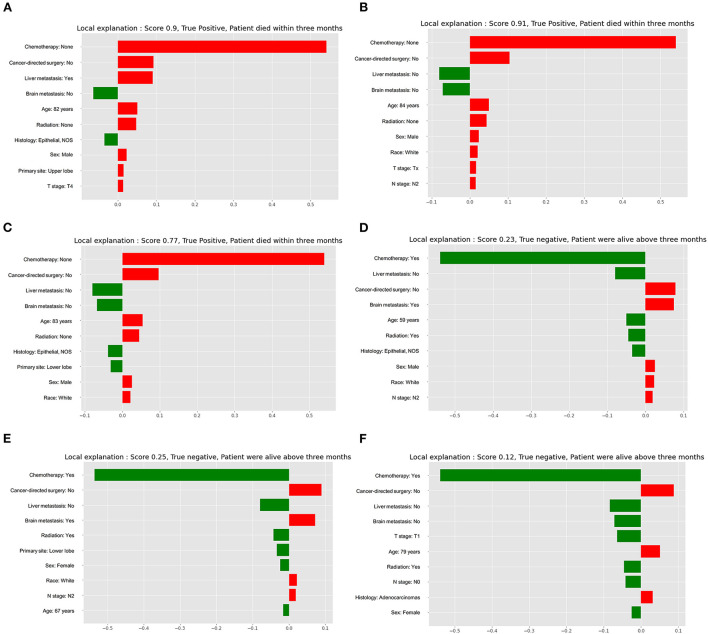
This study enrolled 19,887 lung cancer patients with bone metastases between 2010 and 2018 from a large oncologic database in the United States. According to a ratio of 8:2, the entire patient cohort was randomly assigned to a training ( = 15881, 80%) and validation ( = 4,006, 20%) group. In the training group, prediction models were trained and optimized using six approaches, including logistic regression, XGBoosting machine, random forest, neural network, gradient boosting machine, and decision tree. There were 13 metrics, including the Brier score, calibration slope, intercept-in-large, area under the curve (AUC), and sensitivity, used to assess the model's prediction performance in the validation group. In each metric, the best prediction effectiveness was assigned six points, while the worst was given one point. The model with the highest sum score of the 13 measures was optimal. The model's explainability was performed using the local interpretable model-agnostic explanation (LIME) according to the optimal model. Predictor importance was assessed using HO automatic machine learning. Risk stratification was also evaluated based on the optimal threshold.
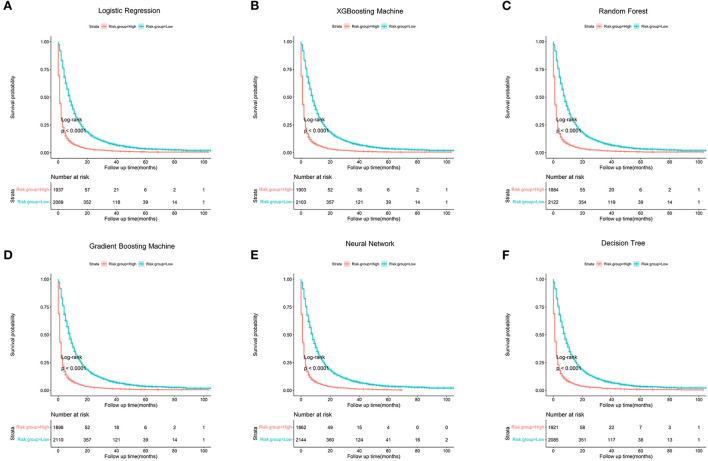
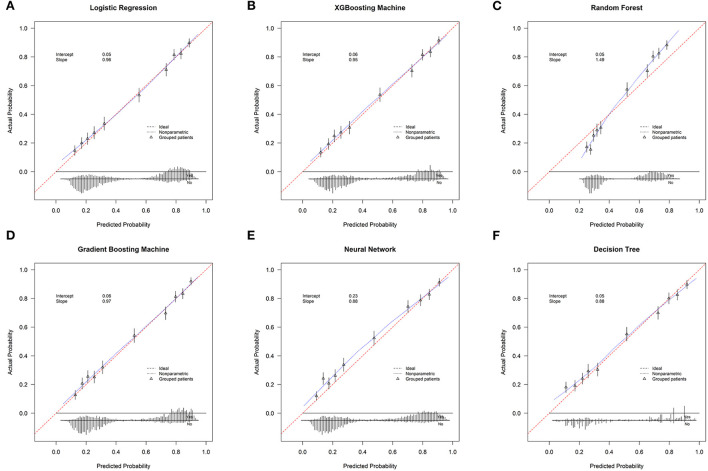
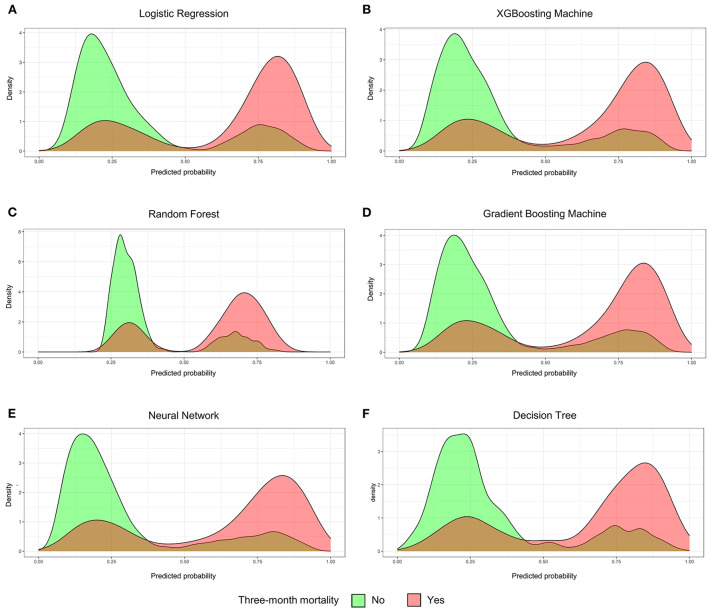
Among all recruited patients, the 3 month mortality was 48.5%. Twelve variables, including age, primary site, histology, race, sex, tumor (T) stage, node (N) stage, brain metastasis, liver metastasis, cancer-directed surgery, radiation, and chemotherapy, were significantly associated with 3 month mortality based on multivariate analysis, and these variables were included for developing prediction models. With the highest sum score of all the measurements, the gradient boosting machine approach outperformed all the other models (62 points), followed by the XGBooting machine approach (59 points) and logistic regression (53). The area under the curve (AUC) was 0.820 (95% confident interval [CI]: 0.807-0.833), 0.820 (95% CI: 0.807-0.833), and 0.815 (95% CI: 0.801-0.828), respectively, calibration slope was 0.97, 0.95, and 0.96, respectively, and accuracy was all 0.772. Explainability of models was conducted to rank the predictors and visualize their contributions to an individual's mortality outcome. The top four important predictors in the population according to HO automatic machine learning were chemotherapy, followed by liver metastasis, radiation, and brain metastasis. Compared to patients in the low-risk group, patients in the high-risk group were more than three times the odds of dying within 3 months ( < 0.001).
Using machine learning techniques, this study offers a number of models, and the optimal model is found after thoroughly assessing and contrasting the prediction performance of each model. The optimal model can be a pragmatic risk prediction tool and is capable of identifying lung cancer patients with bone metastases who are at high risk for 3 month mortality, informing risk counseling, and aiding clinical treatment decision-making. It is better advised for patients in the high-risk group to have radiotherapy alone, the best supportive care, or minimally invasive procedures like cementoplasty.
骨骼是恶性肿瘤扩散最常见的部位之一。预计预后不足 3 个月(早期死亡)的骨转移患者被认为是手术禁忌证。然而,目前文献中的信息限制了我们评估 3 个月死亡率风险可能性的能力。因此,本研究的目的是利用机器学习技术创建一个准确的预测模型,专门针对根据易于获得的临床数据预测肺癌伴骨转移患者 3 个月的死亡率。
本研究纳入了 2010 年至 2018 年期间来自美国一个大型肿瘤数据库的 19887 例肺癌伴骨转移患者。根据 8:2 的比例,将整个患者队列随机分配到训练组(=15881,80%)和验证组(=4006,20%)。在训练组中,使用六种方法(逻辑回归、XGBoosting 机、随机森林、神经网络、梯度提升机和决策树)对预测模型进行训练和优化。有 13 个指标,包括 Brier 评分、校准斜率、截距大、曲线下面积(AUC)和灵敏度,用于评估验证组中模型的预测性能。在每个指标中,最好的预测效果得 6 分,最差的得 1 分。具有最高 13 个指标总和分数的模型是最优的。根据最优模型,使用局部可解释模型不可知解释(LIME)对模型的可解释性进行分析。使用 HO 自动机器学习评估预测器的重要性。还根据最优阈值进行风险分层评估。
在所有入组患者中,3 个月死亡率为 48.5%。根据多变量分析,12 个变量,包括年龄、原发部位、组织学、种族、性别、肿瘤(T)期、淋巴结(N)期、脑转移、肝转移、癌症定向手术、放疗和化疗,与 3 个月死亡率显著相关,并将这些变量纳入预测模型。基于所有测量的最高总分,梯度提升机方法的表现优于其他所有模型(62 分),其次是 XGBooting 机方法(59 分)和逻辑回归(53 分)。曲线下面积(AUC)分别为 0.820(95%置信区间[CI]:0.807-0.833)、0.820(95%CI:0.807-0.833)和 0.815(95%CI:0.801-0.828),校准斜率分别为 0.97、0.95 和 0.96,准确性均为 0.772。对模型进行可解释性分析以对预测器进行排序,并可视化其对个体死亡率结果的贡献。根据 HO 自动机器学习,人群中前四个重要的预测因子是化疗,其次是肝转移、放疗和脑转移。与低危组患者相比,高危组患者在 3 个月内死亡的几率高出三倍以上(<0.001)。
本研究使用机器学习技术提供了多种模型,并通过全面评估和对比每个模型的预测性能,找到了最优模型。最优模型可以作为一种实用的风险预测工具,能够识别出肺癌伴骨转移且 3 个月内死亡风险较高的患者,为风险咨询提供信息,并为临床治疗决策提供支持。建议高危组患者进行单独放疗、最佳支持性护理或微创治疗,如骨水泥成形术。