Morote Juan, Borque-Fernando Ángel, Triquell Marina, Campistol Miriam, Celma Anna, Regis Lucas, Abascal José M, Servian Pol, Planas Jacques, Mendez Olga, Esteban Luis M, Trilla Enrique
Department of Urology and Surgery, Vall d'Hebron Hospital and Universitat Autònoma de Barcelona, 08035 Barcelona, Spain.
Department of Urology, Hospital Miguel Servet, IIS-Aragon, 50009 Zaragoza, Spain.
Cancers (Basel). 2022 Oct 18;14(20):5100. doi: 10.3390/cancers14205100.
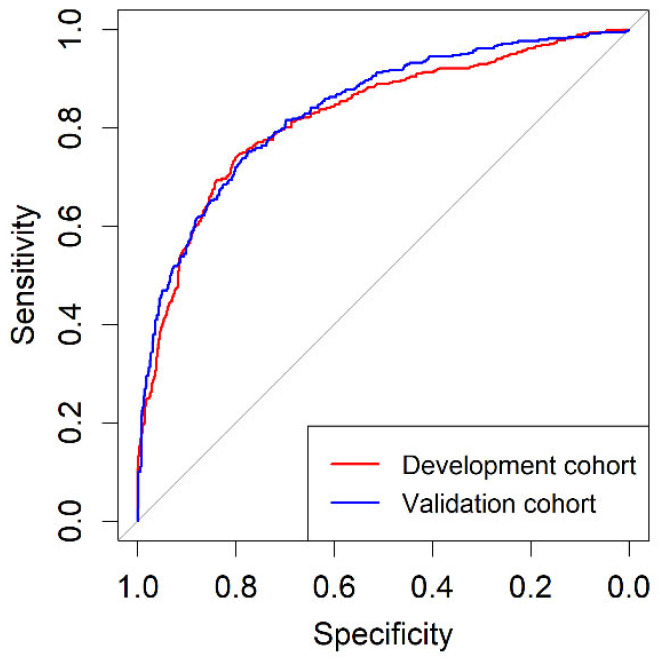
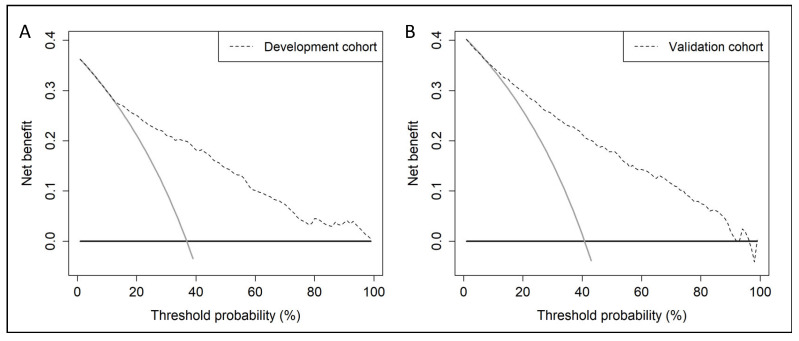
A predictive model including age, PCa family history, biopsy status (initial vs repeat), DRE (normal vs abnormal), serum prostate-specific antigen (PSA), and DRE prostate volume ca-tegory was developed to stratify initial PCa suspicion in 1486 men with PSA > 3 ng/mL and/or abnormal DRE, in whom mpMRI followed; 2- to 4-core TRUS-guided biopsies where Prostate Imaging Report and Data System (PI-RADS) > 3 lesions and/or 12-core TRUS systematic biopsies were performed in one academic institution between 1 January 2016−31 December 2019. The csPCa detection rate, defined as International Society of Uro-Pathology grade group 2 or higher, was 36.9%. An external validation of designed BCN-RC 1 was carried out on 946 men from two other institutions in the same metropolitan area, using the same criteria of PCa suspicion and diagnostic approach, yielded a csPCa detection rate of 40.8%. The areas under the receiver operating characteristic curves of BCN-RC 1 were 0.823 (95% CI: 0.800−0.846) in the development cohort and 0.837 (95% CI: 0.811−0.863) in the validation cohort (p = 0.447). In both cohorts, BCN-RC 1 exhibited net benefit over performing mpMRI in all men from 8 and 12% risk thresholds, respectively. At 0.95 sensitivity of csPCa, the specificities of BCN-RC 1 were 0.24 (95% CI: 0.22−0.26) in the development cohort and 0.34 (95% CI: 0.31−0.37) in the validation cohort (p < 0.001). The percentages of avoided mpMRI scans were 17.2% in the development cohort and 22.3% in the validation cohort, missing between 1.8% and 2% of csPCa among men at risk of PCa. In summary, BCN-RC 1 can stratify initial PCa suspicion, reducing the demand of mpMRI, with an acceptable loss of csPCa.
建立了一个预测模型,该模型纳入了年龄、前列腺癌家族史、活检状态(初次活检与重复活检)、直肠指检(正常与异常)、血清前列腺特异性抗原(PSA)以及直肠指检前列腺体积类别,用于对1486名PSA>3 ng/mL和/或直肠指检异常的男性进行初始前列腺癌怀疑分层,这些男性随后接受了多参数磁共振成像(mpMRI)检查;在2016年1月1日至2019年12月31日期间,在一家学术机构对前列腺影像报告和数据系统(PI-RADS)>3类病变进行了2至4针经直肠超声引导下活检和/或12针经直肠超声系统活检。临床显著前列腺癌(csPCa)的检出率(定义为国际泌尿病理学会分级组2级或更高)为36.9%。使用相同的前列腺癌怀疑标准和诊断方法,对来自同一大都市地区另外两家机构的946名男性进行了设计的BCN-RC 1的外部验证,csPCa检出率为40.8%。在开发队列中,BCN-RC 1的受试者操作特征曲线下面积为0.823(95%CI:0.800−0.846),在验证队列中为0.837(95%CI:0.811−0.863)(p = 0.447)。在两个队列中,BCN-RC 1在风险阈值分别为8%和12%的所有男性中,与进行mpMRI相比均显示出净效益。在csPCa敏感性为0.95时,BCN-RC 1在开发队列中的特异性为0.24(95%CI:0.22−0.26),在验证队列中为0.34(95%CI:0.31−0.37)(p<0.001)。在开发队列中,避免进行mpMRI扫描的百分比为17.2%,在验证队列中为22.3%,在有前列腺癌风险的男性中,遗漏了1.8%至2%的csPCa。总之,BCN-RC 1可以对初始前列腺癌怀疑进行分层,减少对mpMRI的需求,同时csPCa的遗漏率可接受。