Department of Physical Medicine and Rehabilitation, Harvard Medical School, Boston, MA, USA.
Laboratory of SCI, Stem Cell and Recovery Neurobiology Research, Department of Physical Medicine and Rehabilitation, Spaulding Rehabilitation Hospital Network, Mass General Brigham, and Harvard Medical School, 300 1St Avenue, Charlestown Navy Yard, Boston, MA, 02129, USA.
J Neuroinflammation. 2022 Oct 29;19(1):264. doi: 10.1186/s12974-022-02628-2.
People with spinal cord injury (SCI) frequently develop neuropathic pain (NP) that worsens disability and diminishes rehabilitation efficacy. Chronic NP is presently incurable due to poor understanding of underlying mechanisms. We hypothesized that multilocus neuroinflammation (NIF) might be a driver of SCI NP, and tested it by investigating whether NP coexisted with central NIF, neurotransmission (NTM), neuromodulation (NML) and neuroplasticity (NPL) changes post-SCI.
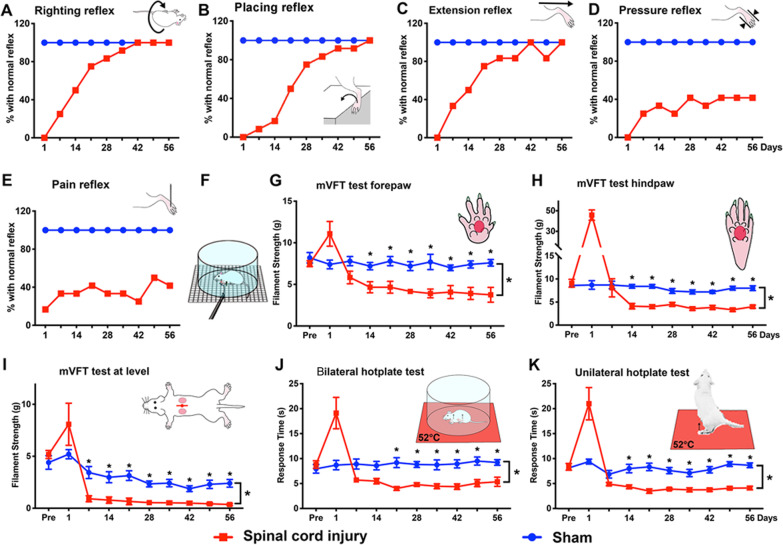
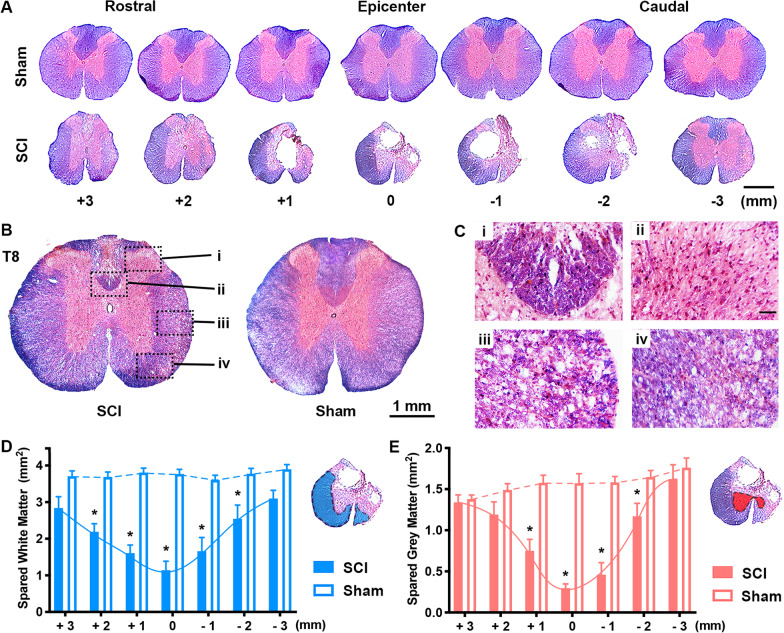
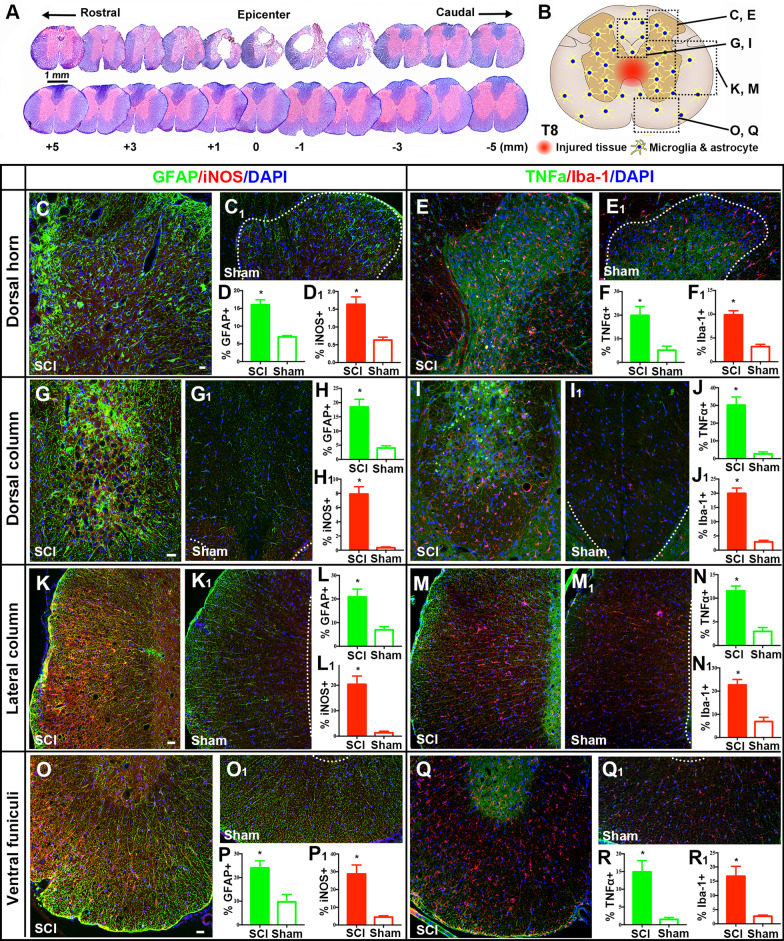
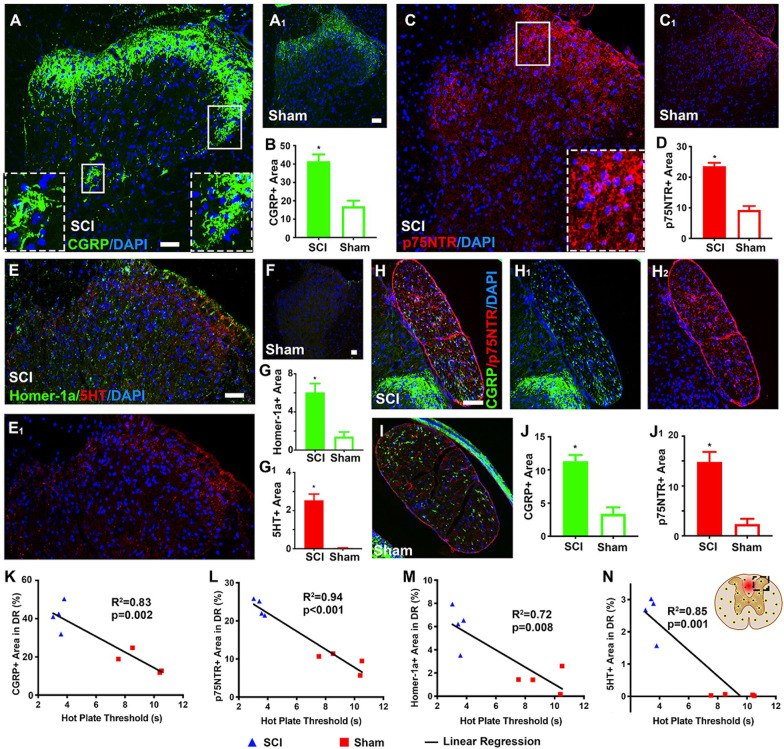
Female Sprague-Dawley rats (230-250 g) with T10 compression or laminectomy were evaluated for physical conditions, coordinated hindlimb functions, neurological reflexes, and mechanical/thermal sensitivity thresholds at 1 day post-injury (p.i.) and weekly thereafter. Eight weeks p.i., central nervous system tissues were histochemically and immunohistochemically characterized for parameters/markers of histopathology and NIF/NTM/NML/NPL. Also analyzed was the correlative relationship between levels of selected biomarkers and thermosensitivity thresholds via statistical linear regression.
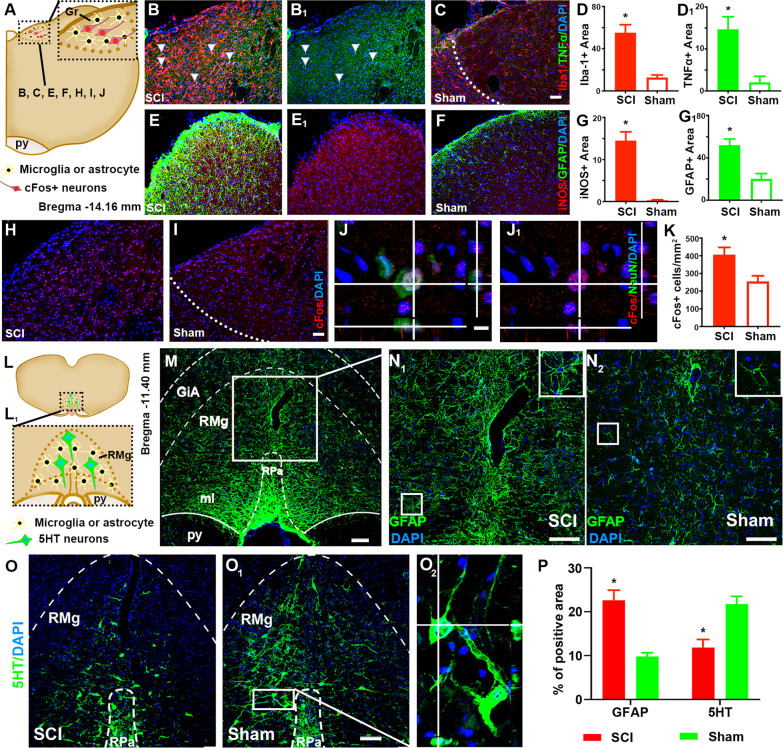
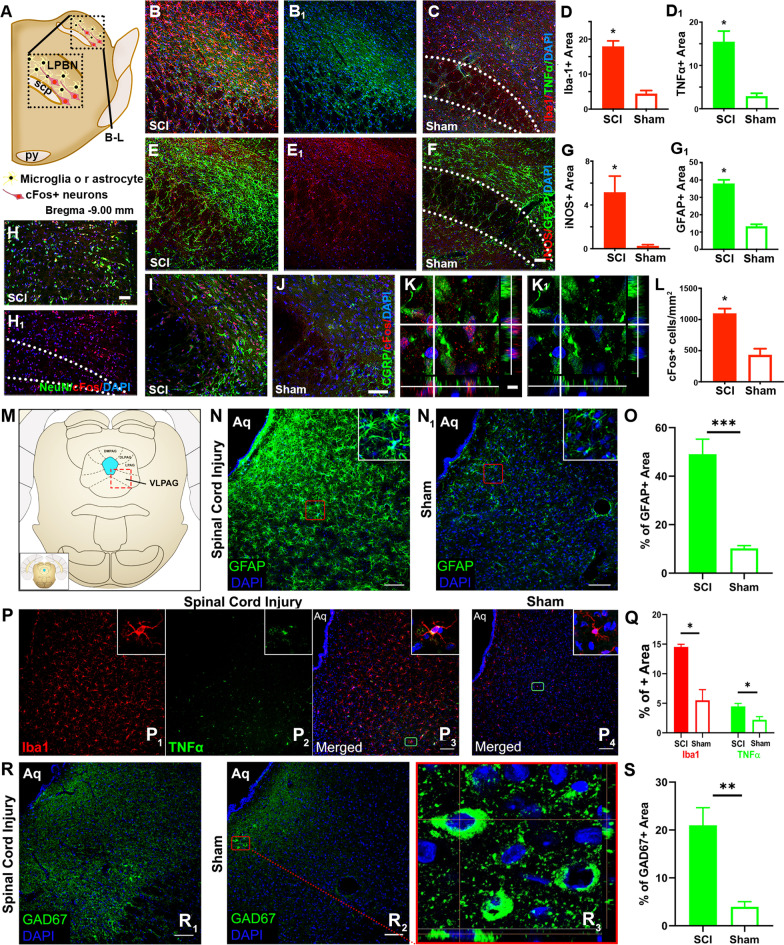
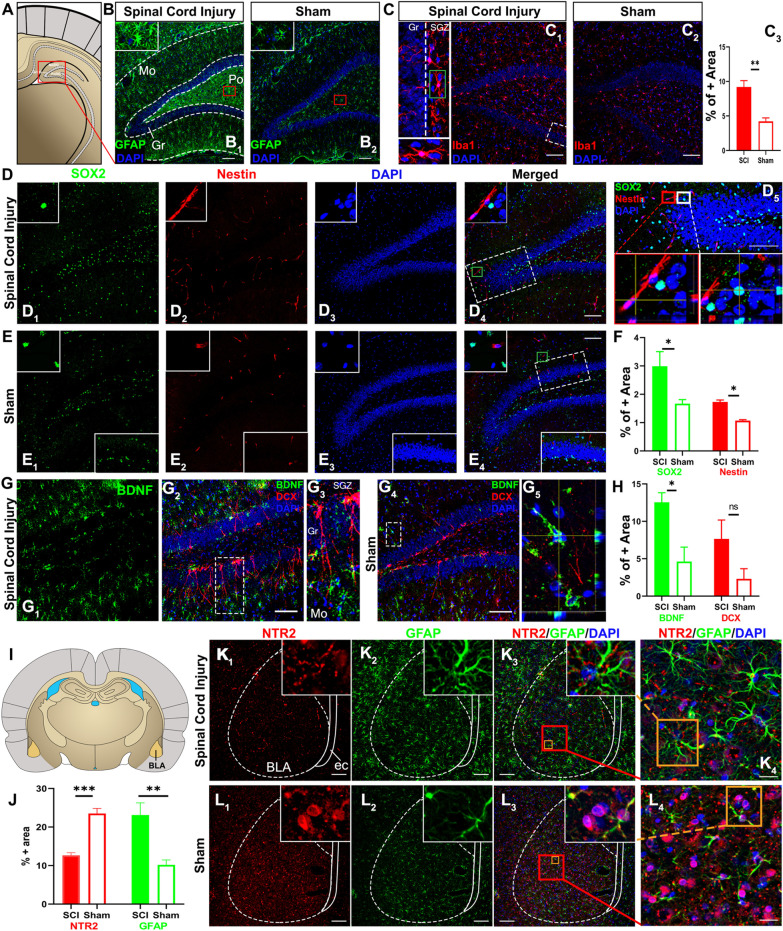
SCI impaired sensorimotor functions, altered reflexes, and produced spontaneous pain signs and hypersensitivity to evoked nociceptive, mechanical, and thermal inputs. Only injured spinal cords exhibited neural lesion, microglia/astrocyte activation, and abnormal expression of proinflammatory cytokines, as well as NIF/NTM/NML/NPL markers. Brains of SCI animals displayed similar pathophysiological signs in the gracile and parabrachial nuclei (GrN and PBN: sensory relay), raphe magnus nucleus and periaqueduct gray (RMN and PAG: pain modulation), basolateral amygdala (BLA: emotional-affective dimension of pain), and hippocampus (HPC: memory/mood/neurogenesis). SCI augmented sensory NTM/NPL (GrN and PBN); increased GAD67 (PAG) level; reduced serotonin (RMN) and fear-off neuronal NTR2 (BLA) expressions; and perturbed neurogenesis (HPC).
T10 compression caused chronic hyperalgesia that coexisted with NIF/NTM/NML/NPL responses at multilevel neuroaxis centers. The data have provided multidimensional biomarkers as new mechanistic leads to profile SCI NP for therapeutic/therapy development.
脊髓损伤(SCI)患者常发生神经病理性疼痛(NP),这会加重残疾并降低康复效果。由于对潜在机制缺乏了解,目前慢性 NP 无法治愈。我们假设多部位神经炎症(NIF)可能是 SCI NP 的驱动因素,并通过研究 SCI 后 NP 是否与中枢 NIF、神经传递(NTM)、神经调节(NML)和神经可塑性(NPL)变化共存来验证这一假设。
230-250 克雌性 Sprague-Dawley 大鼠,T10 受压或椎板切除术,于损伤后 1 天(p.i.)及此后每周评估其身体状况、协调后肢功能、神经反射和机械/热感觉阈值。8 周 p.i.时,对中枢神经系统组织进行组织化学和免疫组织化学分析,以评估组织病理学和 NIF/NTM/NML/NPL 参数/标志物。还通过统计线性回归分析,分析了选定生物标志物水平与热敏阈值之间的相关性。
SCI 损伤了感觉运动功能,改变了反射,并产生了自发性疼痛迹象和对诱发的伤害性、机械性和热输入的超敏反应。只有损伤的脊髓才表现出神经病变、小胶质细胞/星形胶质细胞激活和促炎细胞因子的异常表达,以及 NIF/NTM/NML/NPL 标志物。SCI 动物的大脑在薄束核和臂旁核(GrN 和 PBN:感觉传递)、中缝大核和导水管周围灰质(RMN 和 PAG:疼痛调节)、基底外侧杏仁核(BLA:疼痛的情绪-情感维度)和海马(HPC:记忆/情绪/神经发生)中表现出类似的病理生理学迹象。SCI 增强了感觉 NTM/NPL(GrN 和 PBN);增加了 GAD67(PAG)水平;降低了血清素(RMN)和恐惧神经元 NTR2(BLA)的表达;并扰乱了神经发生(HPC)。
T10 压迫导致慢性痛觉过敏,同时伴有多水平神经轴中心的 NIF/NTM/NML/NPL 反应。这些数据提供了多维生物标志物,为 SCI NP 的治疗/治疗开发提供了新的机制线索。