Department of Surgery, Amsterdam UMC, University of Amsterdam, IBD Unit Ospedale San Raffaele, Meibergdreef 9, 1105 AZ, Amsterdam, the Netherlands.
Gastroenterology and Endoscopy, IBD Unit, IRCCS Ospedale San Raffaele and University Vita-Salute San Raffaele, Milan, Italy.
Int J Colorectal Dis. 2022 Dec;37(12):2491-2499. doi: 10.1007/s00384-022-04280-x. Epub 2022 Nov 11.
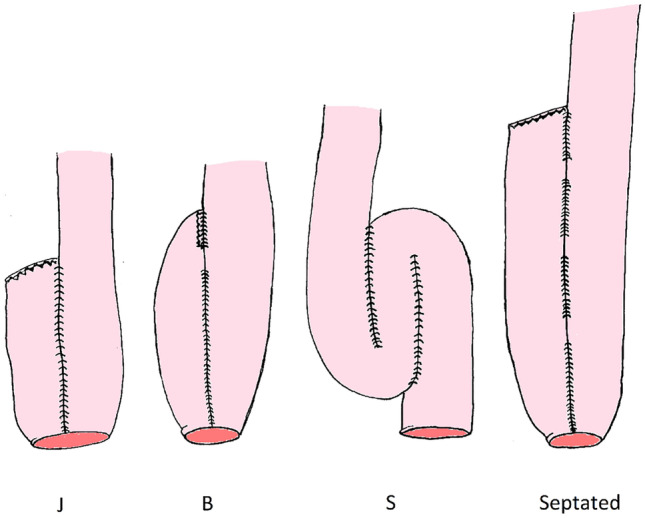
Since the introduction of ileo-pouch anal anastomosis (IPAA) surgery, various pouch designs have been applied. Recently, there has been renewed interest in creating larger pouch designs to reduce defecation frequency after pouch surgery. The aim of this study was to assess chronic pouch failure (PF) rates and causes in alternative S or septated (SP) pouches when compared to J pouches and B- shaped adaptations.
This retrospective cohort study included patients that underwent primary IPAA construction surgery from 1978-2000. Pouch designs were subdivided in J and B (J/B), and larger pouches (S/SP). PF included need for a pouch excision, redo pouch procedure, revisional pouch surgery, or permanent ileostomy surgery. Outcomes of this study were incidence and causes for PF per pouch design group.
Out of 200 patients who underwent IPAA surgery, 19 had an S/SP design and 181 had a J/B design. After a follow-up of 27.0 (IQR 23.3 - 29.0) years, 45/200 (22.5%) patients who underwent IPAA surgery between 1975-2000 developed PF. Some 78.9% of patients with an S/SP pouch developed PF, compared to 16.7% of patients with a J/B pouch (p < 0.01). Mechanical outlet issues occurred more often in S/SP pouches when compared to J/B (42.1% vs. 1.1%, p < 0.01), and were predominantly caused by septal- or pouch wall intussusception and efferent loop kinking (S-pouch).
Despite an inevitable proportion of bias, the current study revealed that S/SP pouches were characterized by an increased PF incidence due to emptying problems after long-term follow-up when compared to J/B pouches. Constructing an S pouch or large septated reservoir at index surgery should therefore be questioned because of a shorter longevity.
自从引入回肠贮袋肛管吻合术(IPAA)以来,已经应用了各种贮袋设计。最近,人们重新产生了设计更大贮袋的兴趣,以减少贮袋手术后的排便频率。本研究的目的是评估与 J 型贮袋和 B 型改型相比,替代 S 型或分隔(SP)贮袋的慢性贮袋失败(PF)发生率和原因。
本回顾性队列研究纳入了 1978 年至 2000 年期间接受初次 IPAA 手术的患者。将贮袋设计分为 J 型和 B 型(J/B)以及较大的贮袋(S/SP)。PF 包括需要切除贮袋、重新进行贮袋手术、修正贮袋手术或永久性回肠造口术。本研究的结果是按贮袋设计组计算 PF 的发生率和原因。
在 200 例接受 IPAA 手术的患者中,有 19 例接受了 S/SP 设计,181 例接受了 J/B 设计。在 27.0(IQR 23.3-29.0)年的随访后,1975-2000 年间接受 IPAA 手术的 200 例患者中有 45 例发生 PF。S/SP 贮袋组发生 PF 的患者比例为 78.9%,而 J/B 贮袋组为 16.7%(p<0.01)。与 J/B 贮袋相比,S/SP 贮袋更常发生机械性出口问题(42.1% vs. 1.1%,p<0.01),主要由隔室或贮袋壁套叠和输出袢扭转(S 型贮袋)引起。
尽管存在不可避免的偏倚,但本研究表明,与 J/B 贮袋相比,S/SP 贮袋在长期随访后由于排空问题而导致 PF 发生率增加。因此,在初次手术时构建 S 型贮袋或大的分隔贮池应受到质疑,因为它们的寿命更短。