Department of Orthopaedic Sports Medicine, Technical University of Munich, Ismaninger Str. 22, 81675, Munich, Germany.
Department of Orthopaedics and Trauma Surgery, Musculoskeletal University Center Munich (MUM), University Hospital, LMU Munich, Munich, Germany.
BMC Musculoskelet Disord. 2022 Dec 9;23(1):1078. doi: 10.1186/s12891-022-05935-0.
There exists a vast number of surgical treatment options for acromioclavicular (AC) joint injuries, and the current literature has yet to determine an equivocally superior treatment. AC joint repair has a long history and dates back to the beginning of the twentieth century.
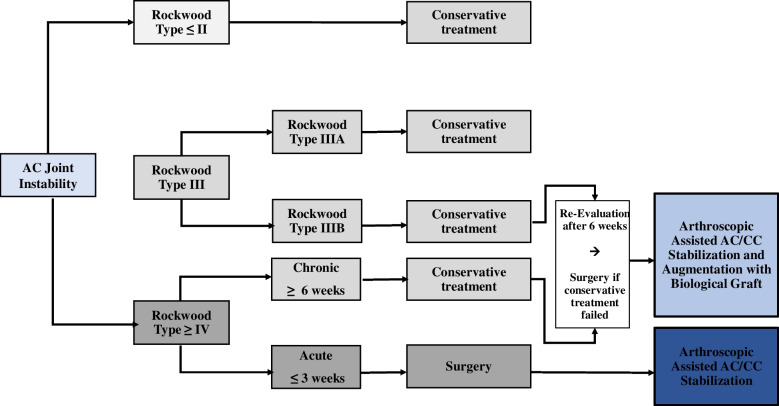
Since then, over 150 different techniques have been described, covering open and closed techniques. Low grade injuries such as Type I-II according to the modified Rockwood classification should be treated conservatively, while high-grade injuries (types IV-VI) may be indicated for operative treatment. However, controversy exists if operative treatment is superior to nonoperative treatment, especially in grade III injuries, as functional impairment due to scapular dyskinesia or chronic pain remains concerning following non-operative treatment. Patients with a stable AC joint without overriding of the clavicle and without significant scapular dysfunction (Type IIIA) may benefit from non-interventional approaches, in contrast to patients with overriding of the clavicle and therapy-resistant scapular dysfunction (Type IIIB). If these patients are considered non-responders to a conservative approach, an anatomic AC joint reconstruction using a hybrid technique should be considered. In chronic AC joint injuries, surgery is indicated after failed nonoperative treatment of 3 to 6 months. Anatomic AC joint reconstruction techniques along with biologic augmentation (e.g. Hybrid techniques, suture fixation) should be considered for chronic high-grade instabilities, accounting for the lack of intrinsic healing and scar-forming potential of the ligamentous tissue in the chronic setting. However, complication and clinical failure rates remain high, which may be a result of technical failures or persistent horizontal and rotational instability.
Future research should focus on addressing horizontal and rotational instability, to restore native physiological and biomechanical properties of the AC joint.
肩锁关节(AC)损伤有大量的手术治疗选择,目前的文献尚未确定一种明确占优的治疗方法。AC 关节修复的历史悠久,可以追溯到 20 世纪初。
从那时起,已经描述了超过 150 种不同的技术,包括开放和闭合技术。对于改良 Rockwood 分类的 I-II 型等低等级损伤,应采用保守治疗,而高等级损伤(类型 IV-VI)可能需要手术治疗。然而,对于手术治疗是否优于非手术治疗,尤其是在 III 级损伤中,存在争议,因为由于肩胛骨运动障碍或慢性疼痛导致的功能障碍在非手术治疗后仍然令人担忧。对于 AC 关节稳定、锁骨无重叠且肩胛骨功能障碍不明显的患者(III 型 A),可能受益于非介入治疗方法,而对于锁骨重叠和治疗抵抗性肩胛骨功能障碍的患者(III 型 B)则不然。如果这些患者被认为对保守治疗方法没有反应,可以考虑采用混合技术进行解剖 AC 关节重建。对于慢性 AC 关节损伤,如果非手术治疗失败 3 至 6 个月,应进行手术。对于慢性高等级不稳定,应考虑解剖 AC 关节重建技术和生物增强(例如混合技术、缝线固定),考虑到韧带组织在慢性环境中缺乏内在愈合和形成疤痕的潜力。然而,并发症和临床失败率仍然很高,这可能是由于技术失败或持续的水平和旋转不稳定所致。
未来的研究应侧重于解决水平和旋转不稳定问题,以恢复 AC 关节的固有生理和生物力学特性。