Frizzelli Annalisa, Di Spigno Francesco, Moderato Luca, Halasz Geza, Aiello Marina, Tzani Panagiota, Manari Gaia, Calzetta Luigino, Pisi Roberta, Pelà Giovanna, Piepoli Massimo, Chetta Alfredo
Department of Medicine and Surgery, University of Parma, 43126 Parma, Italy.
Cardio-Thoracic and Vascular Department, University Hospital of Parma, 43126 Parma, Italy.
J Clin Med. 2022 Dec 13;11(24):7388. doi: 10.3390/jcm11247388.
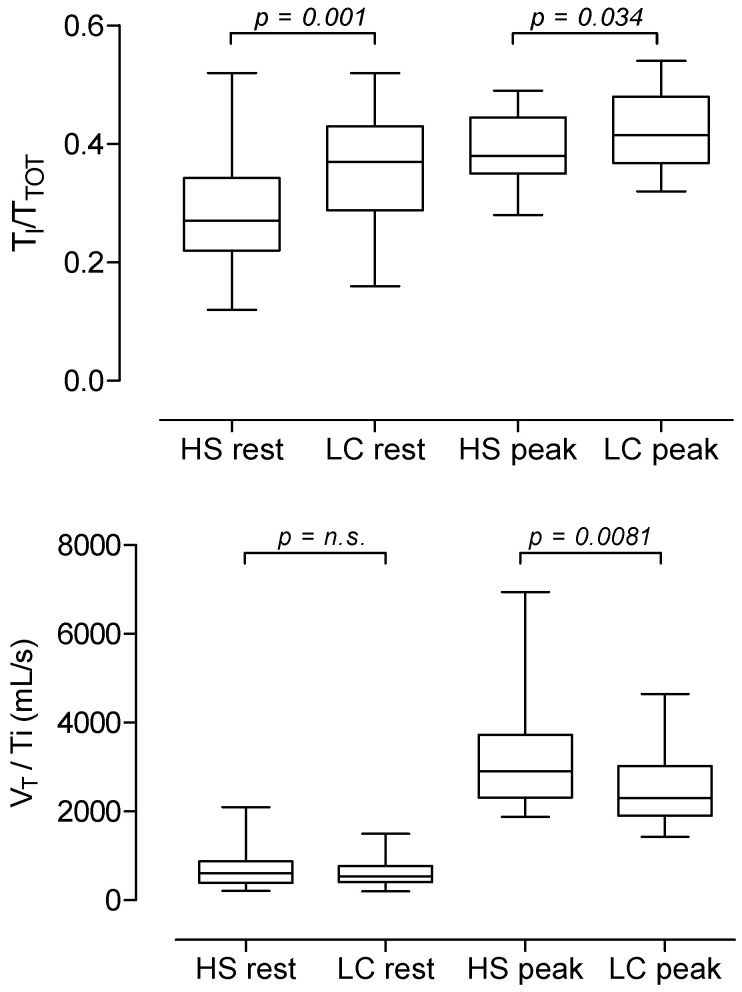
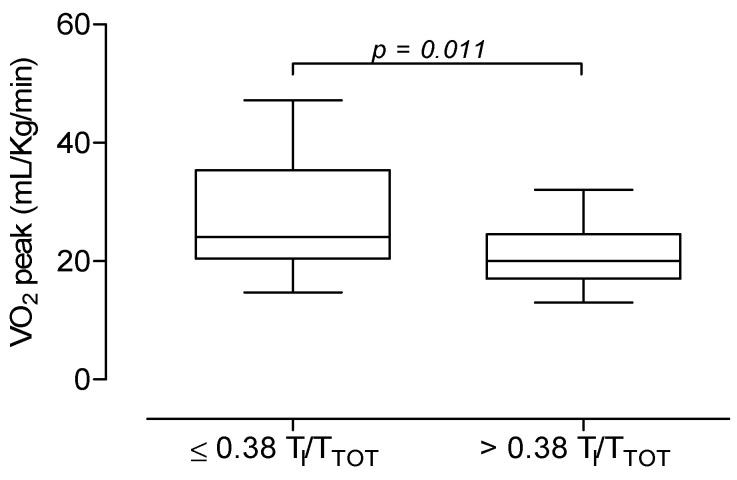
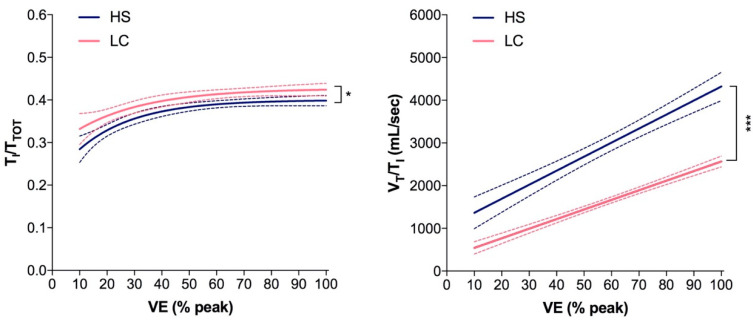
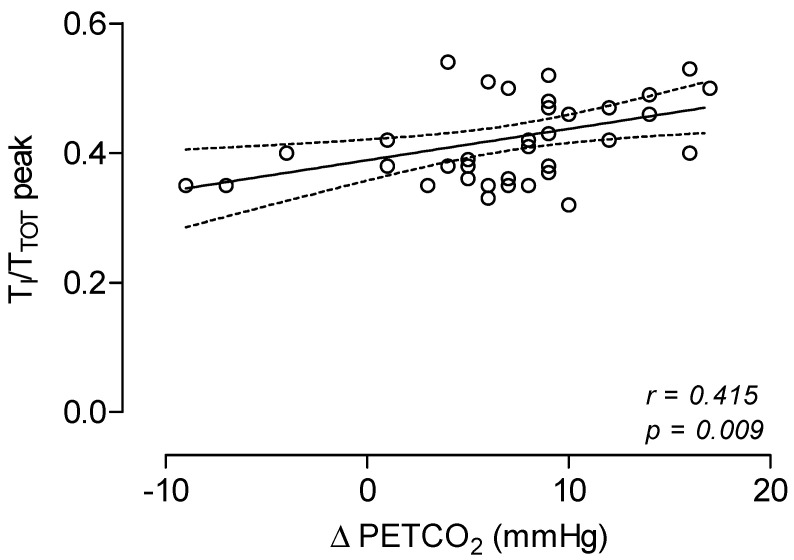
Background: Long-term sequelae, called Long-COVID (LC), may occur after SARS-CoV-2 infection, with unexplained dyspnoea as the most common symptom. The breathing pattern (BP) analysis, by means of the ratio of the inspiratory time (TI) during the tidal volume (VT) to the total breath duration (TI/TTOT) and by the VT/TI ratio, could further elucidate the underlying mechanisms of the unexplained dyspnoea in LC patients. Therefore, we analysed TI/TTOT and VT/TI at rest and during maximal exercise in LC patients with unexplained dyspnoea, compared to a control group. Methods: In this cross-sectional study, we enrolled LC patients with normal spirometry, who were required to perform a cardio-pulmonary exercise test (CPET) for unexplained dyspnoea, lasting at least 3 months after SARS-CoV-2 infection. As a control group, we recruited healthy age and sex-matched subjects (HS). All subjects performed spirometry and CPET, according to standardized procedures. Results: We found that 42 LC patients (23 females) had lower maximal exercise capacity, both in terms of maximal O2 uptake (VO2peak) and workload, compared to 40 HS (22 females) (p < 0.05). LC patients also showed significantly higher values of TI/TTOT at rest and at peak, and lower values in VT/TI at peak (p < 0.05). In LC patients, values of TI/TTOT at peak were significantly related to ∆PETCO2, i.e., the end-tidal pressure of CO2 at peak minus the one at rest (p < 0.05). When LC patients were categorized by the TI/TTOT 0.38 cut-off value, patients with TI/TTOT > 0.38 showed lower values in VO2peak and maximal workload, and greater values in the ventilation/CO2 linear relationship slope than patients with TI/TTOT ≤ 0.38 (p < 0.05). Conclusions: Our findings show that LC patients with unexplained dyspnoea have resting and exertional BP more prone to diaphragmatic fatigue, and less effective than controls. Pulmonary rehabilitation might be useful to revert this unpleasant condition.
新冠病毒(SARS-CoV-2)感染后可能会出现称为“长新冠”(LC)的长期后遗症,其中不明原因的呼吸困难是最常见的症状。通过潮气量(VT)期间吸气时间(TI)与总呼吸持续时间的比值(TI/TTOT)以及VT/TI比值进行呼吸模式(BP)分析,可能会进一步阐明LC患者不明原因呼吸困难的潜在机制。因此,我们分析了不明原因呼吸困难的LC患者在静息状态和最大运动时的TI/TTOT和VT/TI,并与对照组进行了比较。
在这项横断面研究中,我们纳入了肺功能正常的LC患者,这些患者在SARS-CoV-2感染后至少3个月因不明原因呼吸困难而需要进行心肺运动试验(CPET)。作为对照组,我们招募了年龄和性别匹配的健康受试者(HS)。所有受试者均按照标准化程序进行肺功能检查和CPET。
我们发现,与40名HS(22名女性)相比,42名LC患者(23名女性)在最大摄氧量(VO2peak)和工作量方面的最大运动能力较低(p<0.05)。LC患者在静息和峰值时的TI/TTOT值也显著更高,而在峰值时的VT/TI值更低(p<0.05)。在LC患者中,峰值时的TI/TTOT值与∆PETCO2显著相关,即峰值时的呼气末二氧化碳分压减去静息时的呼气末二氧化碳分压(p<0.05)。当根据TI/TTOT 0.38的临界值对LC患者进行分类时,TI/TTOT>0.38的患者在VO2peak和最大工作量方面的值较低,而在通气/二氧化碳线性关系斜率方面的值高于TI/TTOT≤0.38的患者(p<0.05)。
我们的研究结果表明,不明原因呼吸困难的LC患者在静息和运动时的呼吸模式更容易出现膈肌疲劳,且比对照组效率更低。肺康复可能有助于改善这种不良状况。