Unit of Entomology, Department of Parasitology, National Institute of Biomedical Research, Kinshasa, Democratic Republic of the Congo.
Unit of Clinical Pharmacology and Pharmacovigilance, Department of Base Science, Faculty of Medicine, University of Kinshasa, Kinshasa, Democratic Republic of the Congo.
Malar J. 2023 Jan 5;22(1):3. doi: 10.1186/s12936-022-04415-z.
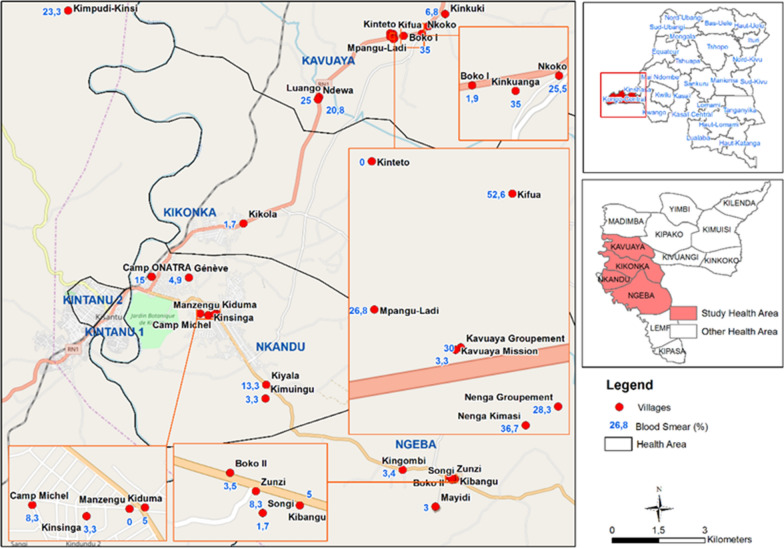
The Democratic Republic of the Congo (DRC) is the second most malaria-affected country in the world with 21,608,681 cases reported in 2019. The Kongo Central (KC) Province has a malaria annual incidence of 163 cases/per 1000 inhabitants which are close to the national average of 153.4/1000. However, the malaria prevalence varies both between and within health zones in this province. The main objective of this study was to describe the epidemiology and transmission of malaria among children aged 0 to 10 years in the 4 highest endemic health areas in Kisantu Health Zone (HZ) of KC in DRC.
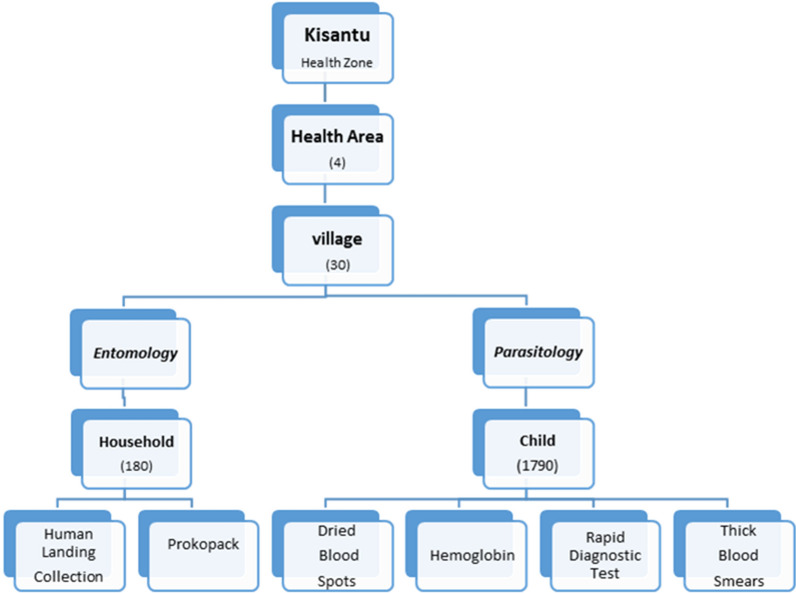
A community-based cross-sectional study was conducted from October to November 2017 using multi-stage sampling. A total of 30 villages in 4 health areas in Kisantu HZ were randomly selected. The prevalence of malaria was measured using a thick blood smear (TBS) and known predictors and associated outcomes were assessed. Data are described and association determinants of malaria infection were analysed.
A total of 1790 children between 0 and 10 years were included in 30 villages in 4 health areas of Kisantu HZ. The overall prevalence in the study area according to the TBS was 14.8% (95% CI: 13.8-16.6; range: 0-53). The mean sporozoite rate in the study area was 4.3% (95% CI: 2.6-6.6). The determination of kdr-west resistance alleles showed the presence of both L1014S and L1014F with 14.6% heterozygous L1014S/L1014F, 84.4% homozygous 1014F, and 1% homozygous 1014S. The risk factors associated with malaria infection were ground or wooden floors aOR: 15.8 (95% CI: 8.6-29.2), a moderate or severe underweight: 1.5 (1.1-2.3) and to be overweight: 1.9 (95% CI: 1.3-2.7).
Malaria prevalence differed between villages and health areas within the same health zone. The control strategy activities must be oriented by the variety in the prevalence and transmission of malaria in different areas. The policy against malaria regarding long-lasting insecticidal nets should be based on the evidence of metabolic resistance.
刚果民主共和国(DRC)是世界上疟疾第二流行的国家,2019 年报告病例 21608681 例。刚果中央省(KC)的疟疾年发病率为每 1000 居民 163 例,接近全国平均水平 153.4/1000。然而,该省不同卫生区之间以及同一卫生区内疟疾的流行率存在差异。本研究的主要目的是描述刚果民主共和国基桑图卫生区(KC)4 个高流行卫生区 0 至 10 岁儿童疟疾的流行病学和传播情况。
2017 年 10 月至 11 月,采用多阶段抽样方法,在基桑图卫生区 4 个卫生区的 30 个村庄进行了一项基于社区的横断面研究。随机选择了基桑图卫生区 4 个卫生区的 30 个村庄。采用厚血涂片(TBS)测量疟疾的患病率,并评估已知的预测因素和相关结局。对数据进行描述,并分析疟疾感染的关联决定因素。
在基桑图卫生区的 4 个卫生区的 30 个村庄共纳入 1790 名 0 至 10 岁儿童。根据 TBS,该研究地区的总患病率为 14.8%(95%CI:13.8-16.6;范围:0-53)。该研究地区的平均孢子体率为 4.3%(95%CI:2.6-6.6)。检测 kdr-west 抗性等位基因表明,存在 L1014S 和 L1014F,杂合子 1014S/L1014F 为 14.6%,纯合子 1014F 为 84.4%,纯合子 1014S 为 1%。与疟疾感染相关的危险因素是地面或木地板(OR:15.8,95%CI:8.6-29.2)、中度或重度体重不足(OR:1.5,95%CI:1.1-2.3)和超重(OR:1.9,95%CI:1.3-2.7)。
疟疾的流行率在不同村庄和同一卫生区内的卫生区之间存在差异。控制策略活动必须针对不同地区疟疾的流行率和传播情况的差异进行定向。针对疟疾的长效驱虫蚊帐政策应基于代谢抗性的证据。