Department of Econometrics, Statistics and Applied Economics, Universitat de Barcelona, Barcelona, Spain
Department of Health Policy, The London School of Economics and Political Science, London, UK.
Emerg Med J. 2023 Apr;40(4):248-256. doi: 10.1136/emermed-2022-212303. Epub 2023 Jan 17.
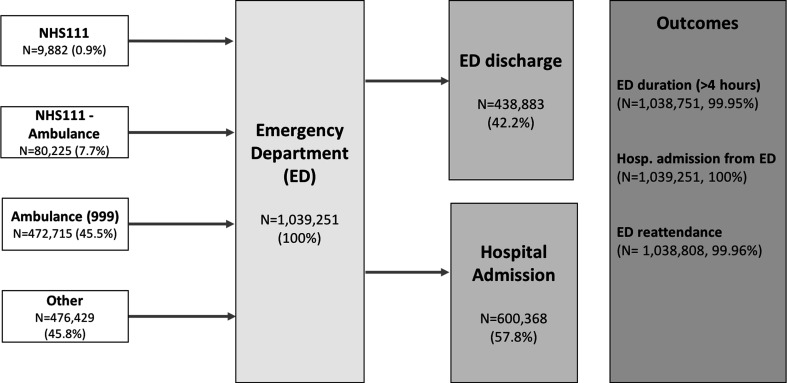
Care for older patients in the ED is an increasingly important issue with the ageing society. To better assess the quality of care in this patient group, we assessed predictors for three outcomes related to ED care: being seen and discharged within 4 hours of ED arrival; being admitted from ED to hospital and reattending the ED within 30 days. We also used these outcomes to identify better-performing EDs.
The CUREd Research Database was used for a retrospective observational study of all 1 039 251 attendances by 368 754 patients aged 75+ years in 18 type 1 EDs in the Yorkshire and the Humber region of England between April 2012 and March 2017. We estimated multilevel logit models, accounting for patients' characteristics and contact with emergency services prior to ED arrival, time variables and the ED itself.
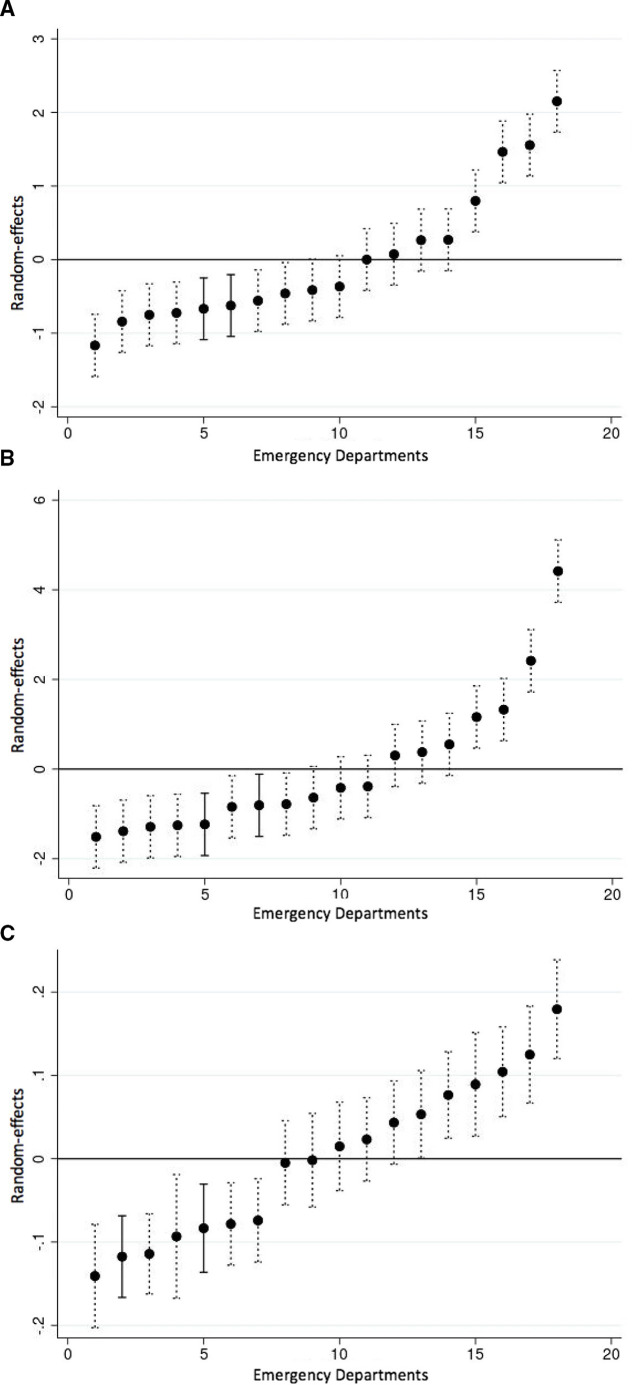
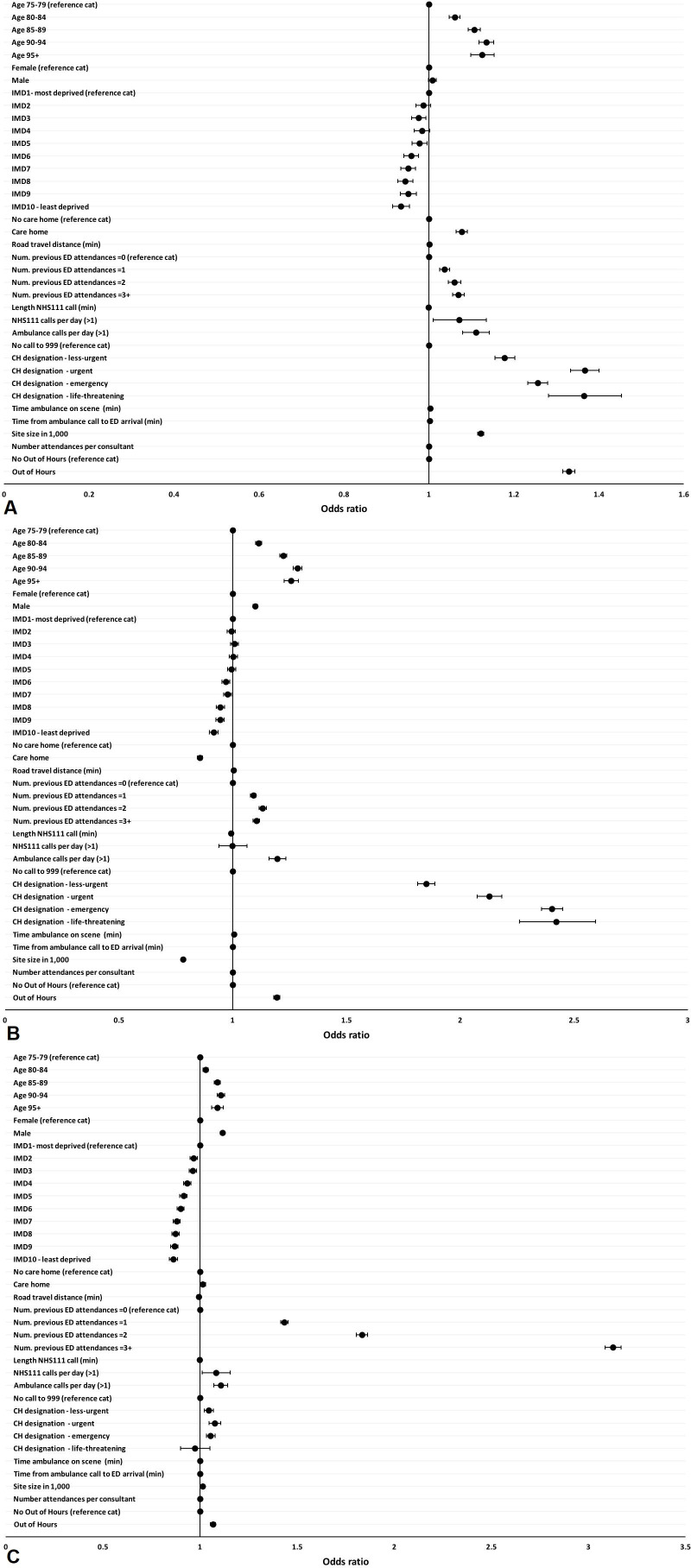
Patients in the oldest category (95+ years vs 75-80 years) were more likely to have a long ED wait (OR=1.13 (95% CI=1.10 to 1.15)), hospital admission (OR=1.26 (95% CI=1.23 to 1.29)) and ED reattendance (OR=1.09 (95% CI=1.06 to 1.12)). Those who had previously attended (3+ vs 0 previous attendances) were more likely to have long wait (OR=1.07 (95% CI=1.06 to 1.08)), hospital admission (OR=1.10 (95% CI=1.09 to 1.12)) and ED attendance (OR=3.13 (95% CI=3.09 to 3.17)). Those who attended out of hours (vs not out of hours) were more likely to have a long ED wait (OR=1.33 (95% CI=1.32 to 1.34)), be admitted to hospital (OR=1.19 (95% CI=1.18 to 1.21)) and have ED reattendance (OR=1.07 (95% CI=1.05 to 1.08)). Those living in less deprived decile (vs most deprived decile) were less likely to have any of these three outcomes: OR=0.93 (95% CI=0.92 to 0.95), 0.92 (95% CI=0.90 to 0.94), 0.86 (95% CI=0.84 to 0.88). These characteristics were not strongly associated with long waits for those who arrived by ambulance. Emergency call handler designation was the strongest predictor of long ED waits and hospital admission: compared with those who did not arrive by ambulance; ORs for these outcomes were 1.18 (95% CI=1.16 to 1.20) and 1.85 (95% CI=1.81 to 1.89) for those designated less urgent; 1.37 (95% CI=1.33 to 1.40) and 2.13 (95% CI=2.07 to 2.18) for urgent attendees; 1.26 (95% CI=1.23 to 1.28) and 2.40 (95% CI=2.36 to 2.45) for emergency attendees; and 1.37 (95% CI=1.28 to 1.45) and 2.42 (95% CI=2.26 to 2.59) for those with life-threatening conditions. We identified two EDs whose patients were less likely to have a long ED, hospital admission or ED reattendance than other EDs in the region.
Age, previous attendance and attending out of hours were all associated with an increased likelihood of exceeding 4 hours in the ED, hospital admission and reattendance among patients over 75 years. These differences were less pronounced among those arriving by ambulance. Emergency call handler designation could be used to identify those at the highest risk of long ED waits, hospital admission and ED reattendance.
随着社会老龄化,对急诊科老年患者的护理成为一个日益重要的问题。为了更好地评估这一患者群体的护理质量,我们评估了与急诊科护理相关的三个结局的预测因素:急诊科到达后 4 小时内得到诊治和出院;从急诊科收治入院和 30 天内再次就诊急诊科。我们还使用这些结局来确定表现更好的急诊科。
利用英格兰约克郡和亨伯地区 18 家 1 型急诊科在 2012 年 4 月至 2017 年 3 月期间的 18 型急诊科 368754 例 75 岁以上患者的 CUREd 研究数据库,对所有 1039251 例就诊进行回顾性观察性研究。我们估计了多水平逻辑模型,考虑了患者的特征以及在急诊科就诊前与紧急服务部门的接触情况、时间变量和急诊科本身。
最年长组(95 岁以上 vs 75-80 岁)的患者在急诊科等待时间较长(OR=1.13(95%CI=1.10-1.15))、住院(OR=1.26(95%CI=1.23-1.29))和急诊科再次就诊(OR=1.09(95%CI=1.06-1.12))的可能性更高。那些之前就诊过(3 次及以上 vs 0 次就诊)的患者在急诊科等待时间较长(OR=1.07(95%CI=1.06-1.08))、住院(OR=1.10(95%CI=1.09-1.12))和急诊科就诊(OR=3.13(95%CI=3.09-3.17))的可能性更高。那些在非工作时间就诊的患者(vs 不在非工作时间就诊)在急诊科等待时间较长(OR=1.33(95%CI=1.32-1.34))、住院(OR=1.19(95%CI=1.18-1.21))和急诊科再次就诊(OR=1.07(95%CI=1.05-1.08))的可能性更高。那些居住在贫困程度较低的十位数(vs 最贫困的十位数)的患者出现这些三个结局的可能性较小:OR=0.93(95%CI=0.92-0.95),0.92(95%CI=0.90-0.94),0.86(95%CI=0.84-0.88)。这些特征与那些通过救护车到达的患者的长等待时间并没有很强的相关性。紧急呼叫处理员的指定是急诊科长等待时间和住院的最强预测因素:与那些没有通过救护车到达的患者相比;这些结局的 OR 分别为 1.18(95%CI=1.16-1.20)和 1.85(95%CI=1.81-1.89);对于指定不太紧急的患者;1.37(95%CI=1.33-1.40)和 2.13(95%CI=2.07-2.18);对于紧急患者;1.26(95%CI=1.23-1.28)和 2.40(95%CI=2.36-2.45);对于有生命危险的患者;1.37(95%CI=1.28-1.45)和 2.42(95%CI=2.26-2.59)。我们确定了两家急诊科,与该地区的其他急诊科相比,这两家急诊科的患者在急诊科、住院和再次就诊的时间都较短。
年龄、既往就诊和非工作时间就诊均与 75 岁以上患者在急诊科的就诊时间延长、住院和再次就诊的可能性增加相关。在通过救护车到达的患者中,这些差异不太明显。紧急呼叫处理员的指定可用于识别那些急诊科等待时间长、住院和再次就诊风险最高的患者。