Department of Environmental Health Sciences, Columbia University, New York, NY, USA.
Department of Epidemiology, Columbia University, New York, NY, USA; CAUSALab, Harvard T H Chan School of Public Health, Boston, MA, USA; Mental Health Network Biomedical Research Center, Madrid, Spain; Mental Health Research Group, Hospital La Paz Institute for Health Research, Madrid, Spain.
Lancet Public Health. 2023 Mar;8(3):e184-e193. doi: 10.1016/S2468-2667(22)00290-0. Epub 2023 Jan 23.
Suicide is one of the leading causes of death in the USA and population risk prediction models can inform decisions on the type, location, and timing of public health interventions. We aimed to develop a prediction model to estimate county-level suicide risk in the USA using population characteristics.
We obtained data on all deaths by suicide reported to the National Vital Statistics System between Jan 1, 2005, and Dec 31, 2019, and age, sex, race, and county of residence of the decedents were extracted to calculate baseline risk. We also obtained county-level annual measures of socioeconomic predictors of suicide risk (unemployment, weekly wage, poverty prevalence, median household income, and population density) and state-level prevalence of major depressive disorder and firearm ownership from US public sources. We applied conditional autoregressive models, which account for spatiotemporal autocorrelation in response and predictors, to estimate county-level suicide risk.
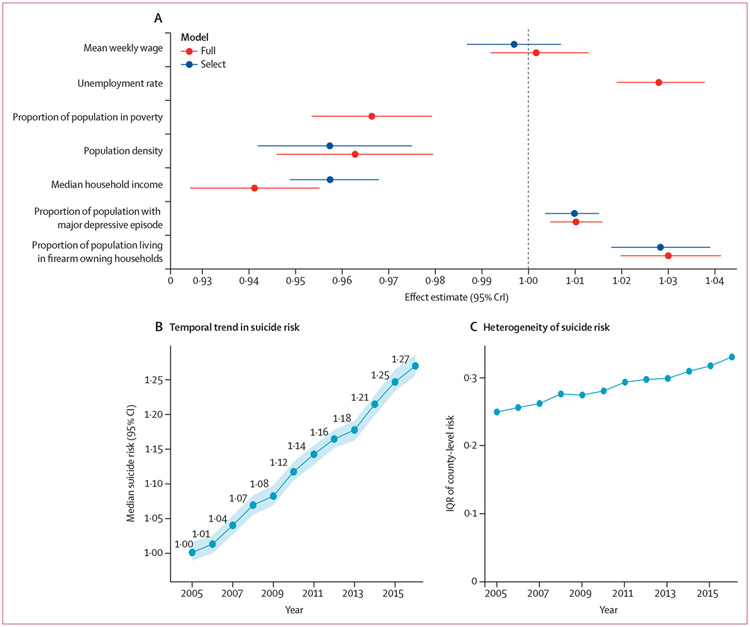
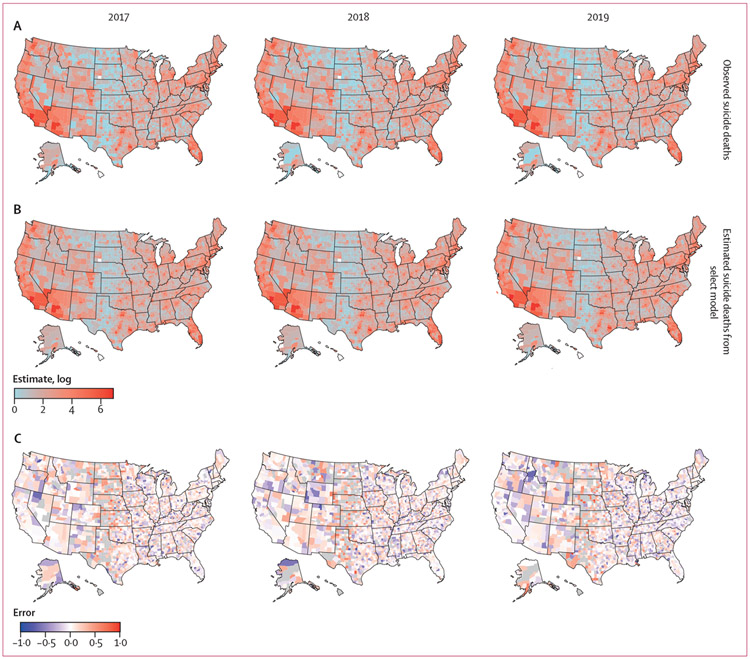
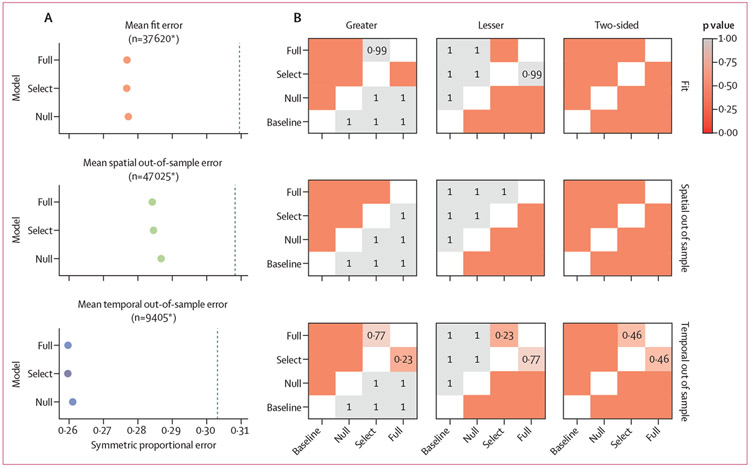
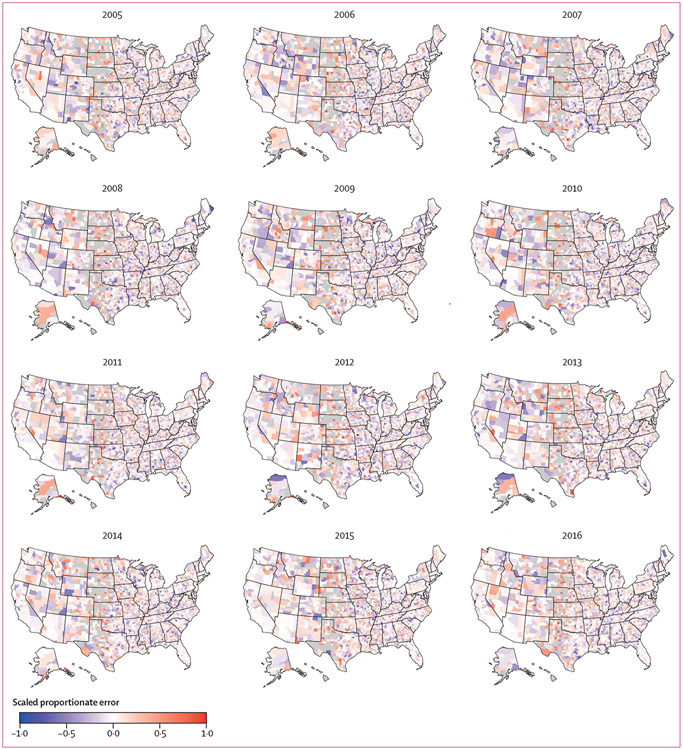
Estimates derived from conditional autoregressive models were more accurate than from models not adjusted for spatiotemporal autocorrelation. Inclusion of suicide risk and protective covariates further reduced errors. Suicide risk was estimated to increase with each SD increase in firearm ownership (2·8% [95% credible interval (CrI) 1·8 to 3·9]), prevalence of major depressive episode (1·0% [0·4 to 1·5]), and unemployment rate (2·8% [1·9 to 3·8]). Conversely, risk was estimated to decrease by 4·3% (-5·1 to -3·2) for each SD increase in median household income and by 4·3% (-5·8 to -2·5) for each SD increase in population density. An increase in the heterogeneity in county-specific suicide risk was also observed during the study period.
Area-level characteristics and the conditional autoregressive models can estimate population-level suicide risk. Availability of near real-time situational data are necessary for the translation of these models into a surveillance setting. Monitoring changes in population-level risk of suicide could help public health agencies select and deploy targeted interventions quickly.
US National Institute of Mental Health.
自杀是美国主要死因之一,人群风险预测模型可辅助决策公共卫生干预的类型、地点和时机。本研究旨在开发一种使用人群特征来预测美国县级自杀风险的预测模型。
我们获取了 2005 年 1 月 1 日至 2019 年 12 月 31 日期间向国家生命统计系统报告的所有自杀死亡数据,并提取了死者的年龄、性别、种族和居住县信息,以计算基线风险。此外,我们还从美国公共资源中获取了县级年度自杀风险社会经济预测指标(失业率、周薪、贫困率、家庭收入中位数和人口密度)和州级主要抑郁障碍和枪支拥有率的患病率。我们应用条件自回归模型,该模型考虑了反应和预测因子的时空自相关,以估计县级自杀风险。
条件自回归模型估计的结果比未调整时空自相关的模型更准确。纳入自杀风险和保护因素进一步降低了误差。自杀风险被估计随枪支拥有率每增加一个标准差而增加(2.8%[95%可信区间(CrI)1.8 至 3.9%])、主要抑郁发作的患病率(1.0%[0.4 至 1.5%])和失业率(2.8%[1.9 至 3.8%])。相反,家庭收入中位数每增加一个标准差,风险估计下降 4.3%(-5.1 至-3.2%),人口密度每增加一个标准差,风险估计下降 4.3%(-5.8 至-2.5%)。在研究期间,县级特定自杀风险的异质性也有所增加。
区域特征和条件自回归模型可估计人群水平的自杀风险。需要近实时的情境数据才能将这些模型转化为监测环境。监测人群自杀风险的变化可以帮助公共卫生机构快速选择和部署有针对性的干预措施。
美国国家心理健康研究所。