Department of Epidemiology and Biostatistics, School of Public Health, Imperial College London, London, United Kingdom.
MRC Centre for Environment and Health, Imperial College London, London, United Kingdom.
PLoS Med. 2019 Jul 23;16(7):e1002856. doi: 10.1371/journal.pmed.1002856. eCollection 2019 Jul.
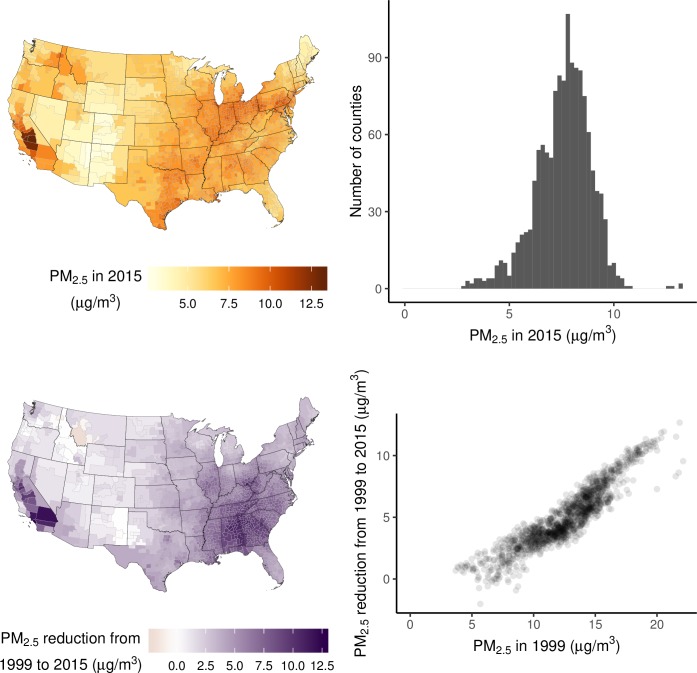
Exposure to fine particulate matter pollution (PM2.5) is hazardous to health. Our aim was to directly estimate the health and longevity impacts of current PM2.5 concentrations and the benefits of reductions from 1999 to 2015, nationally and at county level, for the entire contemporary population of the contiguous United States.
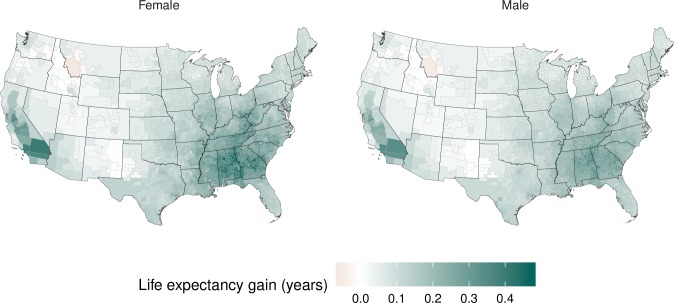
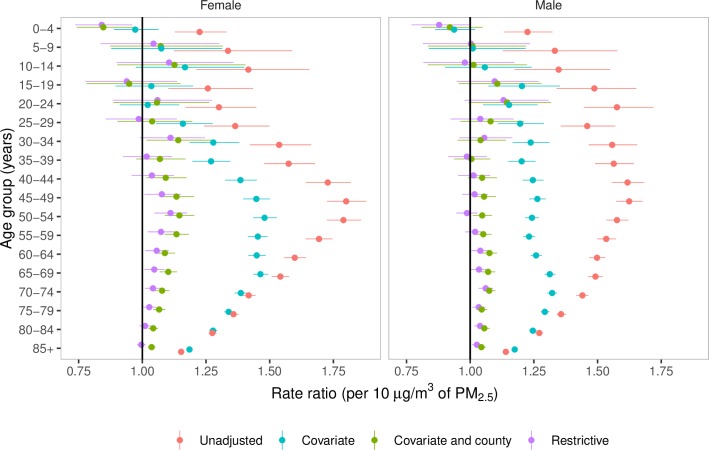
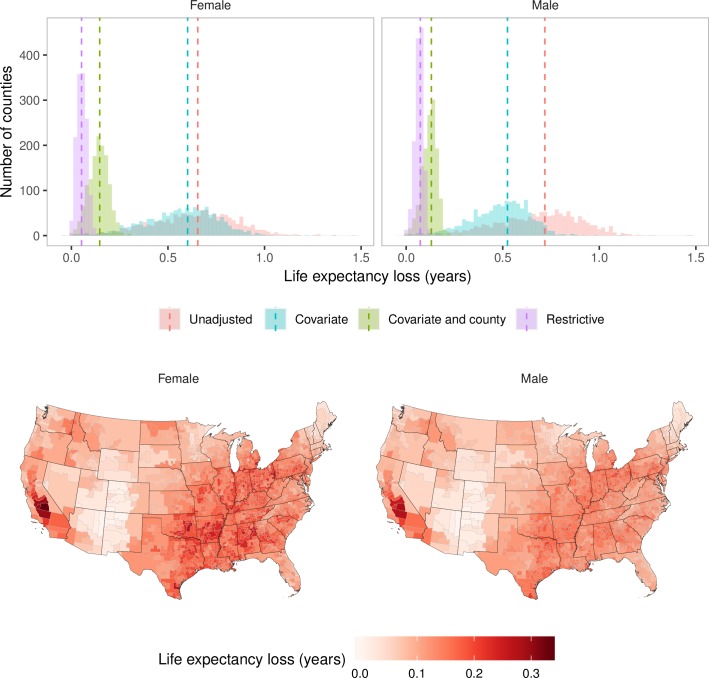
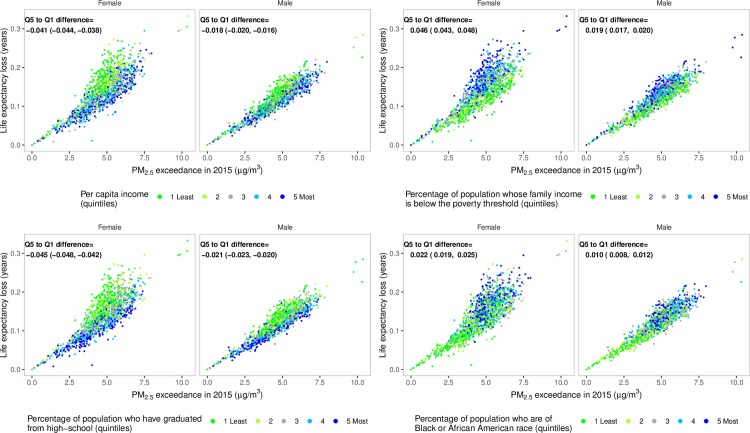
We used vital registration and population data with information on sex, age, cause of death, and county of residence. We used four Bayesian spatiotemporal models, with different adjustments for other determinants of mortality, to directly estimate mortality and life expectancy loss due to current PM2.5 pollution and the benefits of reductions since 1999, nationally and by county. The covariates included in the adjusted models were per capita income; percentage of population whose family income is below the poverty threshold, who are of Black or African American race, who have graduated from high school, who live in urban areas, and who are unemployed; cumulative smoking; and mean temperature and relative humidity. In the main model, which adjusted for these covariates and for unobserved county characteristics through the use of county-specific random intercepts, PM2.5 pollution in excess of the lowest observed concentration (2.8 μg/m3) was responsible for an estimated 15,612 deaths (95% credible interval 13,248-17,945) in females and 14,757 deaths (12,617-16,919) in males. These deaths would lower national life expectancy by an estimated 0.15 years (0.13-0.17) for women and 0.13 years (0.11-0.15) for men. The life expectancy loss due to PM2.5 was largest around Los Angeles and in some southern states such as Arkansas, Oklahoma, and Alabama. At any PM2.5 concentration, life expectancy loss was, on average, larger in counties with lower income and higher poverty rate than in wealthier counties. Reductions in PM2.5 since 1999 have lowered mortality in all but 14 counties where PM2.5 increased slightly. The main limitation of our study, similar to other observational studies, is that it is not guaranteed for the observed associations to be causal. We did not have annual county-level data on other important determinants of mortality, such as healthcare access and quality and diet, but these factors were adjusted for with use of county-specific random intercepts.
According to our estimates, recent reductions in particulate matter pollution in the USA have resulted in public health benefits. Nonetheless, we estimate that current concentrations are associated with mortality impacts and loss of life expectancy, with larger impacts in counties with lower income and higher poverty rate.
细颗粒物污染(PM2.5)暴露对健康有害。我们的目的是直接估计当前 PM2.5 浓度对健康和寿命的影响,以及 1999 年至 2015 年期间的减少量所带来的效益,范围覆盖整个美国的所有当代人口和各个县。
我们使用了与性别、年龄、死因和居住县有关的人口登记和人口数据。我们使用了四个贝叶斯时空模型,对其他死亡率决定因素进行了不同的调整,以直接估计当前 PM2.5 污染导致的死亡率和预期寿命损失,以及自 1999 年以来的减少量,范围覆盖全国和各个县。调整后的模型包括人均收入、家庭收入低于贫困线的人口比例、非裔美国人、高中及以上学历、居住在城市地区和失业人口比例、累计吸烟量以及平均温度和相对湿度。在主要模型中,我们通过使用县特定的随机截距来调整这些协变量以及未观察到的县特征,将超过最低观察浓度(2.8μg/m3)的 PM2.5 污染归因于估计的 15612 名女性死亡(95%可信区间 13248-17945)和 14757 名男性死亡(12617-16919)。这些死亡将使女性的全国预期寿命缩短约 0.15 年(0.13-0.17),男性缩短约 0.13 年(0.11-0.15)。PM2.5 造成的预期寿命损失在洛杉矶及其周边地区和阿肯色州、俄克拉荷马州和阿拉巴马州等一些南部州最大。在任何 PM2.5 浓度下,收入较低和贫困率较高的县的预期寿命损失平均大于富裕县。自 1999 年以来,PM2.5 的减少降低了除 14 个 PM2.5 略有增加的县以外的所有县的死亡率。与其他观察性研究一样,我们研究的主要限制是不能保证观察到的关联是因果关系。我们没有关于其他重要死亡率决定因素的年度县一级数据,如医疗保健的可及性和质量以及饮食,但我们使用县特定的随机截距来调整这些因素。
根据我们的估计,美国最近减少的颗粒物污染带来了公共卫生效益。尽管如此,我们估计目前的浓度与死亡率影响和预期寿命损失有关,收入较低和贫困率较高的县影响更大。