Barberio Julie, Kim Seoyoung C, Roh Miin, Lewis James D, Desai Rishi J
Division of Pharmacoepidemiology and Pharmacoeconomics, Brigham and Women's Hospital, Harvard Medical School, Boston, Massachusetts.
Division of Rheumatology, Immunology and Allergy, Brigham and Women's Hospital, Harvard Medical School, Boston, Massachusetts.
Crohns Colitis 360. 2020 Jun 4;2(3):otaa041. doi: 10.1093/crocol/otaa041. eCollection 2020 Jul.
Inflammatory bowel disease (IBD) patients may develop anterior uveitis.
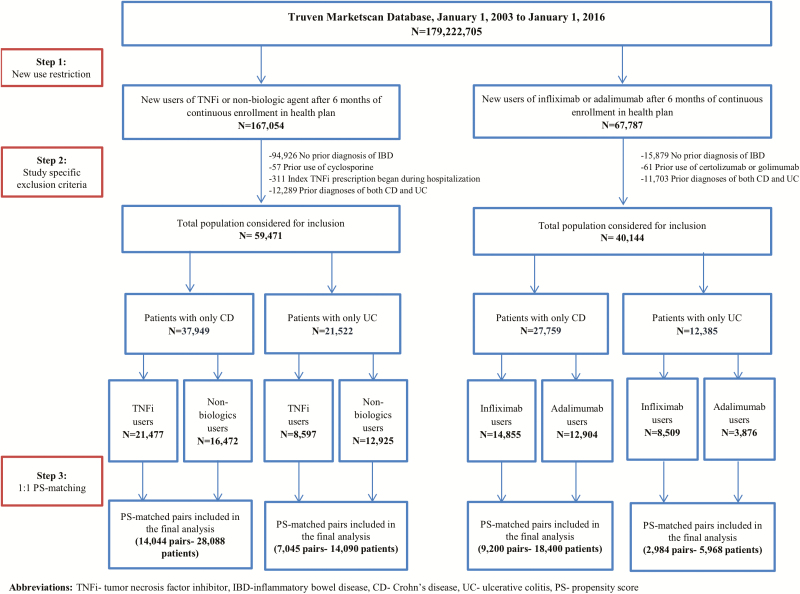
An observational cohort of IBD patients followed new users of (1) tumor necrosis factor inhibitor versus nonbiologic agents or (2) adalimumab versus infliximab until occurrence of anterior uveitis or treatment change/discontinuation. Cox-proportional hazards models estimated hazard ratios in propensity score-matched cohorts of Crohn disease or ulcerative colitis patients.
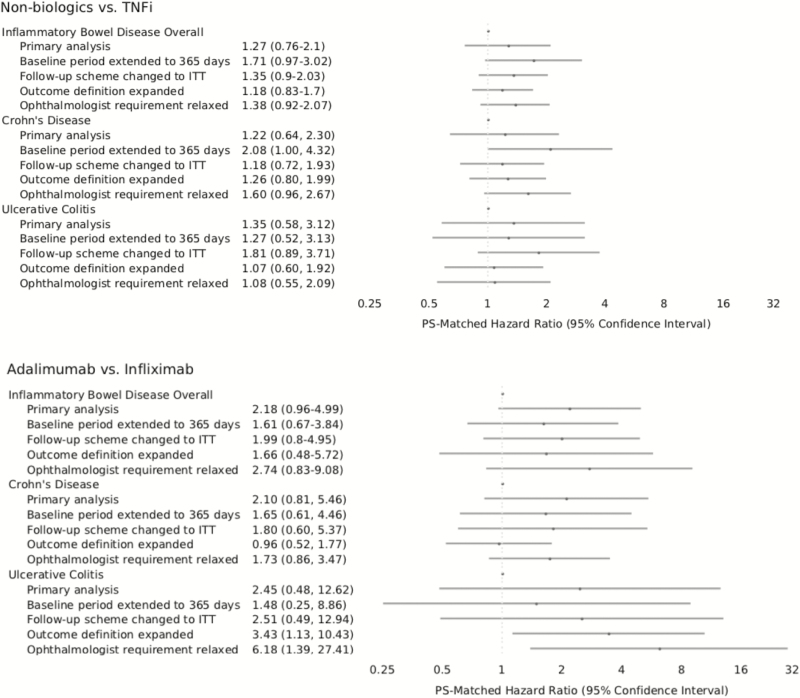
No statistically significant differences in the risk of uveitis were observed between initiators of nonbiologics and tumor necrosis factor inhibitor. Effect estimates for adalimumab versus infliximab were highly imprecise due to limited outcomes.
Uveitis risk was not different between IBD patients treated with immunosuppressives.
炎症性肠病(IBD)患者可能会发生前葡萄膜炎。
一个IBD患者的观察性队列对(1)肿瘤坏死因子抑制剂新使用者与非生物制剂使用者或(2)阿达木单抗与英夫利昔单抗的新使用者进行随访,直至发生前葡萄膜炎或治疗改变/停药。Cox比例风险模型估计了克罗恩病或溃疡性结肠炎患者倾向评分匹配队列中的风险比。
非生物制剂使用者与肿瘤坏死因子抑制剂使用者之间,葡萄膜炎风险未观察到统计学上的显著差异。由于结局有限,阿达木单抗与英夫利昔单抗的效应估计极不精确。
接受免疫抑制剂治疗的IBD患者之间,葡萄膜炎风险无差异。