Medical Intensive Care Unit, Henri Mondor University Hospital, APHP, 1 Rue Gustave Eiffel, 94010, Créteil Cedex, France.
IAME UMR 1137, INSERM, Paris University, 75018, Paris, France.
Crit Care. 2023 Mar 13;27(1):108. doi: 10.1186/s13054-023-04325-9.
Despite antiviral therapy (ART), 800,000 deaths still occur yearly and globally due to HIV infection. In parallel with the good virological control and the aging of this population, multiple comorbidities [HIV-associated-non-AIDS (HANA) conditions] may now be observed.
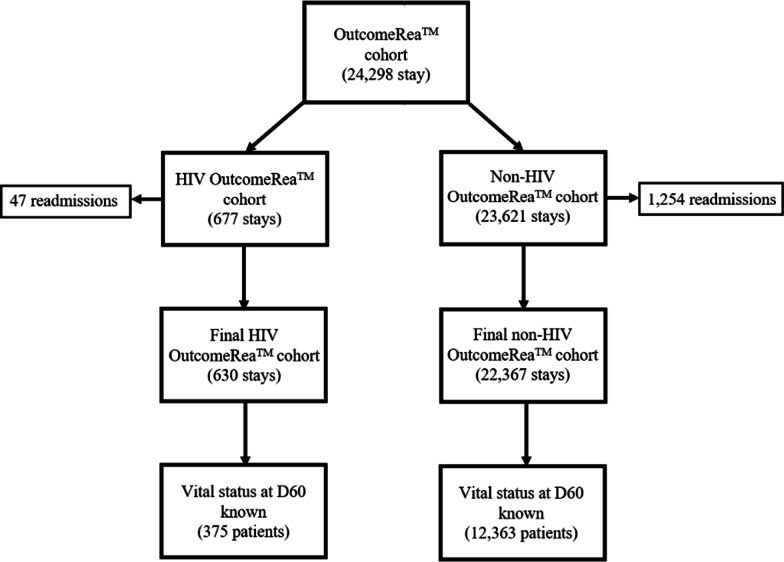
HIV adult patients hospitalized in intensive care unit (ICU) from all the French region from university and non-university hospital who participate to the OutcomeRea™ database on a voluntary basis over a 24-year period.
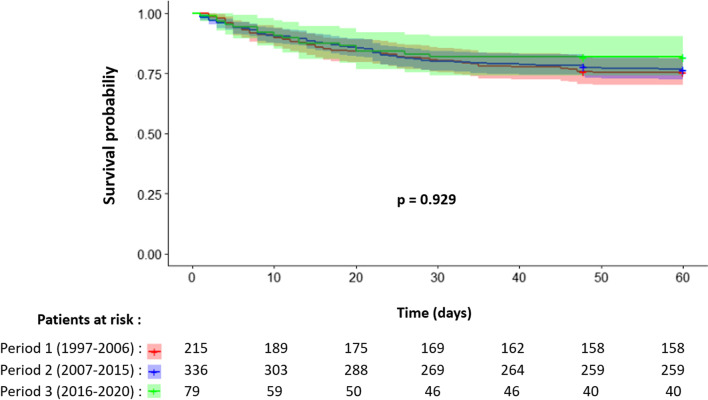
Of the 24,298 stays registered, 630 (2.6%) were a first ICU stay for HIV patients. Over time, the mean age and number of comorbidities (diabetes, renal and respiratory history, solid neoplasia) of patients increased. The proportion of HIV diagnosed on ICU admission decreased significantly, while the median duration of HIV disease as well as the percentage of ART-treated patients increased. The distribution of main reasons for admission remained stable over time (acute respiratory distress > shock > coma). We observed a significant drop in the rate of active opportunistic infection on admission, while the rate of active hemopathy (newly diagnosed or relapsed within the last 6 months prior to admission to ICU) qualifying for AIDS increased-nonsignificantly-with a significant increase in the anticancer chemotherapy administration in ICU. Admissions for HANA or non-HIV reasons were stable over time. In multivariate analysis, predictors of 60-day mortality were advanced age, chronic liver disease, past chemotherapy, sepsis-related organ failure assessment score > 4 at admission, hospitalization duration before ICU admission > 24 h, AIDS status, but not the period of admission.
Whereas the profile of ICU-admitted HIV patients has evolved over time (HIV better controlled but more associated comorbidities), mortality risk factors remain stable, including AIDS status.
尽管有抗病毒治疗(ART),但每年仍有 80 万人因 HIV 感染而死亡,这是全球性的问题。随着该人群病毒学控制良好和老龄化,现在可能会观察到多种合并症[与 HIV 相关的非艾滋病(HANA)状况]。
在 24 年的时间里,所有法国地区的大学和非大学医院的 HIV 成年患者自愿参与了 OutcomeRea™数据库,该数据库记录了所有入住重症监护病房(ICU)的患者。
在登记的 24298 例住院中,有 630 例(2.6%)是 HIV 患者的首次 ICU 住院。随着时间的推移,患者的平均年龄和合并症数量(糖尿病、肾脏和呼吸系统病史、实体瘤)增加。在 ICU 入院时诊断出 HIV 的比例显著下降,而 HIV 疾病的中位持续时间以及接受 ART 治疗的患者比例增加。主要入院原因的分布在一段时间内保持稳定(急性呼吸窘迫>休克>昏迷)。我们观察到入院时活动性机会性感染的发生率显著下降,而在 ICU 入院前 6 个月内新诊断或复发的活动性血液病(符合 AIDS 标准)的比例略有增加-在 ICU 中接受抗癌化疗的人数显著增加。由于 HANA 或非 HIV 原因入院的人数在一段时间内保持稳定。多变量分析显示,60 天死亡率的预测因素是年龄较大、慢性肝病、既往化疗、入院时的脓毒症相关器官衰竭评估评分>4、ICU 入院前的住院时间>24 小时、艾滋病状态,但不是入院时间。
尽管 ICU 收治的 HIV 患者的情况随时间发生了变化(HIV 得到了更好的控制,但合并症更多),但包括艾滋病状态在内的死亡风险因素保持稳定。