Kelley Sarah, Evans M D R, Kelley Jonathan
Department of Data Science and Innovation, Child Trends, Bethesda, MD USA.
Department of Sociology, University of Nevada, Reno, NV USA.
Appl Res Qual Life. 2023;18(1):115-162. doi: 10.1007/s11482-023-10149-0. Epub 2023 Mar 4.
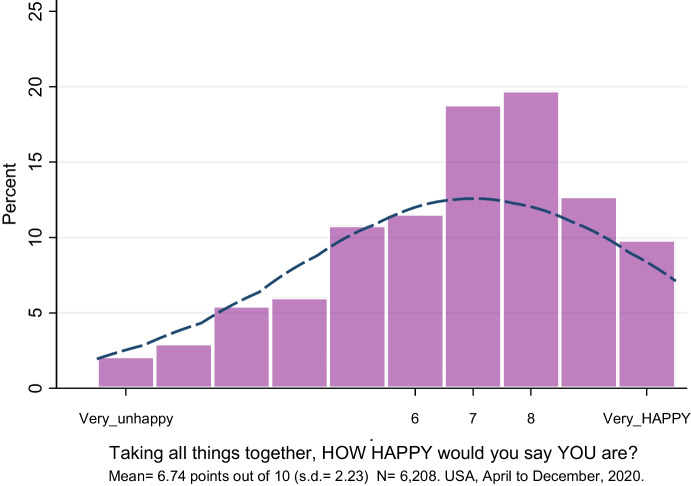
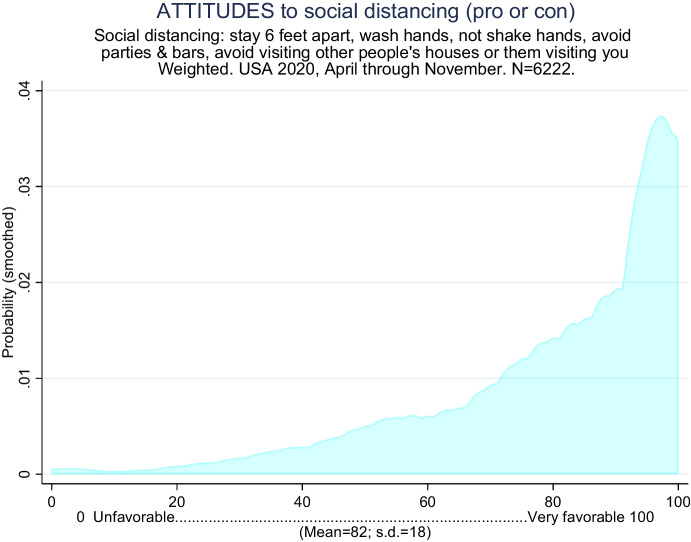
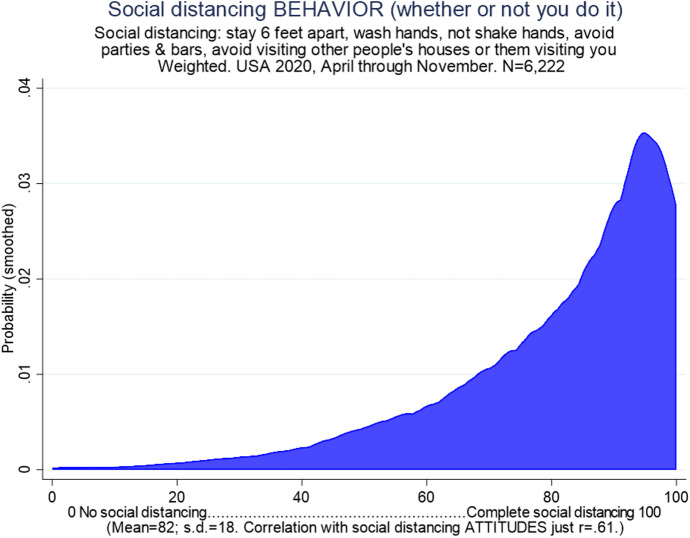
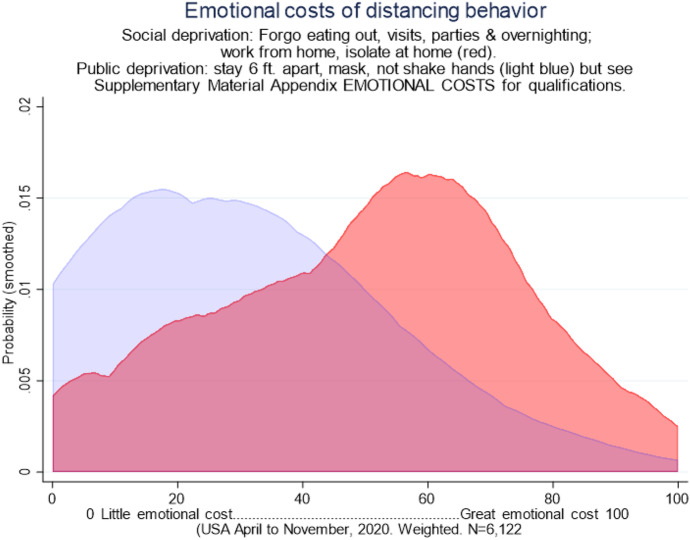
To inhibit the spread of COVID-19 Public health officials stress, and governments often require, restrictions on social interaction ("social distancing"). While the medical benefits are clear, important questions remain about these measures' downsides: How bitter is this medicine? Ten large non-probability internet-based surveys between April and November 2020, weighted statistically to reflect the US population in age, education, and religious background and excluding respondents who even occasionally role-played rather than giving their own true views; = 6,223. Pre-epidemic data from 2017-2019, = 4,032. Reliable multiple-item scales including subjective wellbeing (2 European Quality of Life Survey items, Cronbach's alpha = .85); distancing attitudes (5 items, alpha = .87); distancing behavior e.g., standing 6' apart in public (5 items, alpha = .80); emotional cost of distancing and restrictions on social interaction (8-12 items, alpha = .94); and an extensive suite of controls (19 variables). Descriptive statistics, OLS regression, structural equation models. Subjective wellbeing is greater for those who approve of distancing, for those who practice distancing, and particularly for those whose distancing attitudes and behavior are congruent, either both in favor or both opposed (multiplicative interaction). The emotional cost of distancing is strongly tied to wellbeing and is heterogeneous, with some disliking distancing much more than others. An SEM model suggests causality: that emotional costs strongly reduce wellbeing but not vice-versa. During the epidemic, COVID issues constitute two of the top 5 influences on wellbeing, behind only subjective health and religious belief and tied with income. All this is net of family background, religious origins, age, ethnicity, race, gender, rural residence, education, occupational status, marriage, unemployment, income, health, religion, and political party.
The online version contains supplementary material available at 10.1007/s11482-023-10149-0.
为抑制新冠病毒的传播,公共卫生官员强调且政府常常要求对社交互动加以限制(“社交距离”)。虽然其医学益处显而易见,但这些措施的负面影响仍存在重要问题:这种“药”有多苦?2020年4月至11月期间开展了10项基于互联网的大型非概率调查,经统计加权以反映美国人口的年龄、教育程度和宗教背景,并排除那些哪怕偶尔进行角色扮演而非给出自己真实观点的受访者;样本量 = 6223。2017 - 2019年的疫情前数据,样本量 = 4032。可靠的多项目量表包括主观幸福感(2项欧洲生活质量调查问卷项目,克朗巴哈系数α = 0.85);社交距离态度(5项,α = 0.87);社交距离行为,例如在公共场合保持6英尺距离(5项,α = 0.80);社交距离和社交互动限制的情感成本(8 - 12项,α = 0.94);以及一系列广泛的控制变量(19个变量)。描述性统计、普通最小二乘法回归、结构方程模型。对于那些赞成社交距离的人、践行社交距离的人,尤其是那些社交距离态度和行为一致(要么都赞成要么都反对,乘法交互作用)的人,主观幸福感更高。社交距离的情感成本与幸福感紧密相关且存在异质性,有些人比其他人更讨厌社交距离。一个结构方程模型表明存在因果关系:情感成本会强烈降低幸福感,但反之则不然。在疫情期间,新冠相关问题是对幸福感影响最大的前5个因素中的两个,仅次于主观健康和宗教信仰,与收入并列。所有这些都是在扣除家庭背景、宗教出身、年龄、种族、民族、性别、农村居住情况、教育程度、职业地位、婚姻状况、失业情况、收入、健康状况、宗教信仰和政党等因素后得出的。
在线版本包含可在10.1007/s11482 - 023 - 10149 - 0获取的补充材料。