De Nardi Andrigo Barboza, de Oliveira Massoco Salles Gomes Cristina, Fonseca-Alves Carlos Eduardo, de Paiva Felipe Noleto, Linhares Laís Calazans Menescal, Carra Gabriel João Unger, Dos Santos Horta Rodrigo, Ruiz Sueiro Felipe Augusto, Jark Paulo Cesar, Nishiya Adriana Tomoko, de Carvalho Vasconcellos Carmen Helena, Ubukata Rodrigo, Batschinski Karen, Sobral Renata Afonso, Fernandes Simone Crestoni, Biondi Luiz Roberto, De Francisco Strefezzi Ricardo, Matera Julia Maria, Rangel Marcelo Monte Mor, Dos Anjos Denner Santos, Brunner Carlos Henrique Maciel, Laufer-Amorim Renee, Cadrobbi Karine Germano, Cirillo Juliana Vieira, Martins Mauro Caldas, de Paula Reis Filho Nazilton, Silva Lessa Diego Fernando, Portela Roberta, Scarpa Carneiro Carolina, Ricci Lucas Sílvia Regina, Fukumasu Heidge, Feliciano Marcus Antônio Rossi, Gomes Quitzan Juliany, Dagli Maria Lucia Zaidan
Department of Veterinary Clinic and Surgery, Universidade Estadual Paulista (UNESP), Jaboticabal 14884-900, Brazil.
Department of Pathology, School of Veterinary Medicine and Animal Science, Universidade de São Paulo (USP), São Paulo 05508-900, Brazil.
Cancers (Basel). 2023 Mar 29;15(7):2025. doi: 10.3390/cancers15072025.
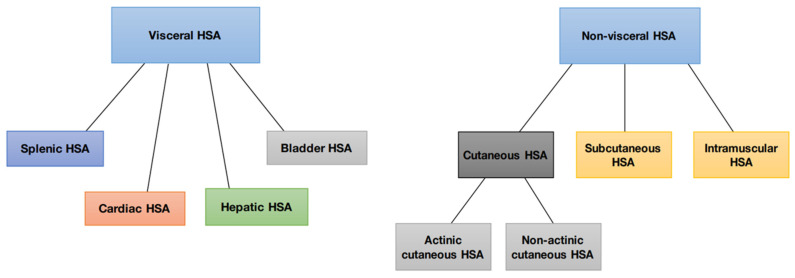
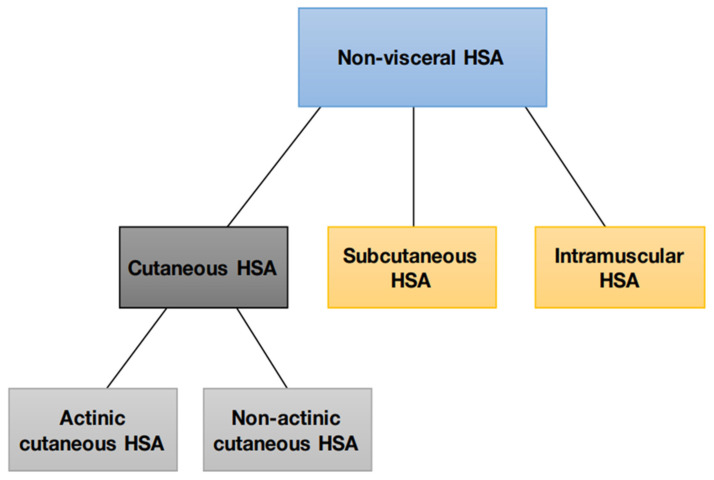
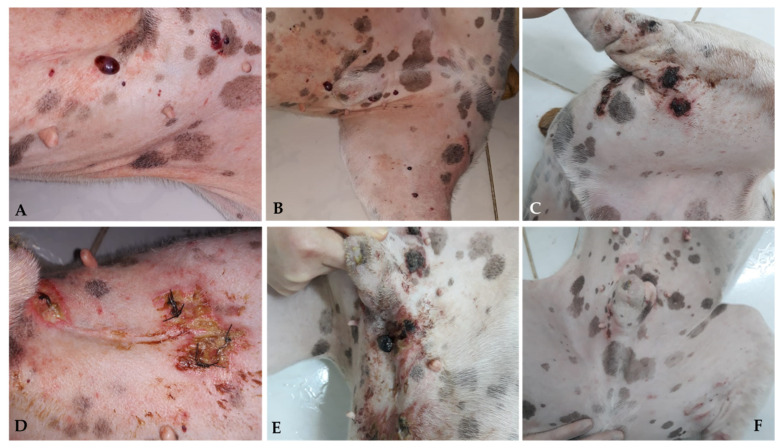
Hemangiosarcoma is a mesenchymal neoplasm originating in the endothelial cells of blood vessels; they can be classified as non-visceral and visceral types. Non-visceral hemangiosarcomas can affect the skin, subcutaneous tissues, and muscle tissues; visceral hemangiosarcomas can affect the spleen, liver, heart, lungs, kidneys, oral cavity, bones, bladder, uterus, tongue, and retroperitoneum. Among domestic species, dogs are most affected by cutaneous HSA. Cutaneous HSA represents approximately 14% of all HSA diagnosed in this species and less than 5% of dermal tumors, according to North American studies. However, Brazilian epidemiological data demonstrate a higher prevalence, which may represent 27 to 80% of all canine HSAs and 13.9% of all skin neoplasms diagnosed in this species. Cutaneous HSA most commonly affects middle-aged to elderly dogs (between 8 and 15 years old), with no gender predisposition for either the actinic or non-actinic forms. The higher prevalence of cutaneous HSA in some canine breeds is related to lower protection from solar radiation, as low skin pigmentation and hair coverage lead to greater sun exposure. Actinic changes, such as solar dermatosis, are frequent in these patients, confirming the influence of solar radiation on the development of this neoplasm. There are multiple clinical manifestations of hemangiosarcoma in canines. The diagnostic approach and staging classification of cutaneous HSAs are similar between the different subtypes. The definitive diagnosis is obtained through histopathological analysis of incisional or excisional biopsies. Cytology can be used as a presurgical screening test; however, it has little diagnostic utility in cases of HSA because there is a high risk of blood contamination and sample hemodilution. Surgery is generally the treatment of choice for dogs with localized non-visceral HSA without evidence of metastatic disease. Recently, electrochemotherapy (ECT) has emerged as an alternative therapy for the local ablative treatment of different neoplastic types; the use of radiotherapy for the treatment of dogs with cutaneous HSA is uncommon. There is greater consensus in the literature regarding the indications for adjuvant chemotherapy in subcutaneous and muscular HSA; doxorubicin is the most frequently used antineoplastic agent for subcutaneous and muscular subtypes and can be administered alone or in combination with other drugs. Other therapies include antiangiogenic therapy, photodynamic therapy, the association of chemotherapy with the metronomic dose, targeted therapies, and natural products. The benefits of these therapies are presented and discussed. In general, the prognosis of splenic and cardiac HSA is unfavorable. As a challenging neoplasm, studies of new protocols and treatment modalities are necessary to control this aggressive disease.
血管肉瘤是一种起源于血管内皮细胞的间叶性肿瘤;可分为非内脏型和内脏型。非内脏型血管肉瘤可累及皮肤、皮下组织和肌肉组织;内脏型血管肉瘤可累及脾脏、肝脏、心脏、肺、肾脏、口腔、骨骼、膀胱、子宫、舌头和腹膜后。在驯养动物中,犬最易患皮肤型血管肉瘤。根据北美研究,皮肤型血管肉瘤约占该物种所有确诊血管肉瘤的14%,占皮肤肿瘤的比例不到5%。然而,巴西的流行病学数据显示其患病率更高,可能占所有犬血管肉瘤的27%至80%,占该物种所有确诊皮肤肿瘤的13.9%。皮肤型血管肉瘤最常发生于中年至老年犬(8至15岁),光化性或非光化性形式均无性别倾向。某些犬种皮肤型血管肉瘤患病率较高与对太阳辐射的防护较低有关,因为皮肤色素沉着少和毛发覆盖少会导致更多阳光暴露。这些患者经常出现光化性改变,如日光性皮炎,证实了太阳辐射对该肿瘤发生发展的影响。犬血管肉瘤有多种临床表现。不同亚型皮肤型血管肉瘤的诊断方法和分期分类相似。通过切开活检或切除活检的组织病理学分析可获得确诊。细胞学可作为术前筛查试验;然而,在血管肉瘤病例中其诊断价值不大,因为存在血液污染和样本血液稀释的高风险。对于局部非内脏型且无转移证据的犬血管肉瘤,手术通常是首选治疗方法。最近,电化学疗法(ECT)已成为不同肿瘤类型局部消融治疗的替代疗法;皮肤型血管肉瘤犬使用放射治疗并不常见。关于皮下和肌肉型血管肉瘤辅助化疗的适应证,文献中有更多共识;阿霉素是皮下和肌肉亚型最常用的抗肿瘤药物,可单独使用或与其他药物联合使用。其他治疗方法包括抗血管生成治疗、光动力治疗、低剂量化疗联合、靶向治疗和天然产物。本文介绍并讨论了这些治疗方法的益处。一般来说,脾脏和心脏型血管肉瘤的预后不佳。作为一种具有挑战性的肿瘤,需要研究新的方案和治疗方式来控制这种侵袭性疾病。