Nasu Izumi, Kondo Masahiro, Uozumi Ryuji, Takada Shinya, Nawata Shuichi, Iihara Hirotoshi, Okumura Yohei, Takemoto Masashi, Mino Kozo, Sasaki Tadanori, Hirose Chiemi, Aomori Tohru, Shimano Rena, Maeno Ken, Oizumi Satoshi, Kusumoto Sojiro, Ohno Yasushi, Ikemura Shinnosuke, Takai Daiya, Hara Azusa, Kawazoe Hitoshi, Nakamura Tomonori
Division of Pharmaceutical Care Sciences, Keio University Graduate School of Pharmaceutical Sciences, 1-5-30 Shibakoen, Minato-ku, Tokyo 105-8512, Japan.
Department of Pharmacy, Toranomon Hospital, 2-2-2 Toranomon, Minato-ku, Tokyo 105-8470, Japan.
J Cancer. 2023 Mar 11;14(5):676-688. doi: 10.7150/jca.80517. eCollection 2023.
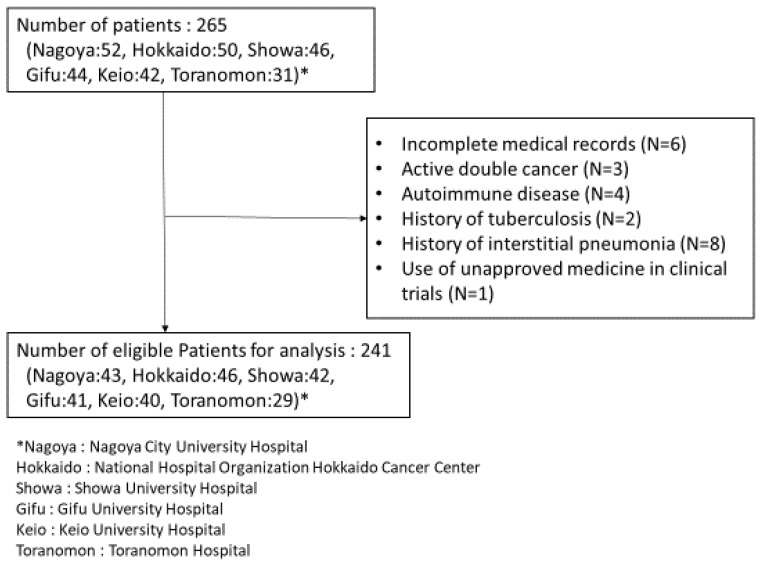
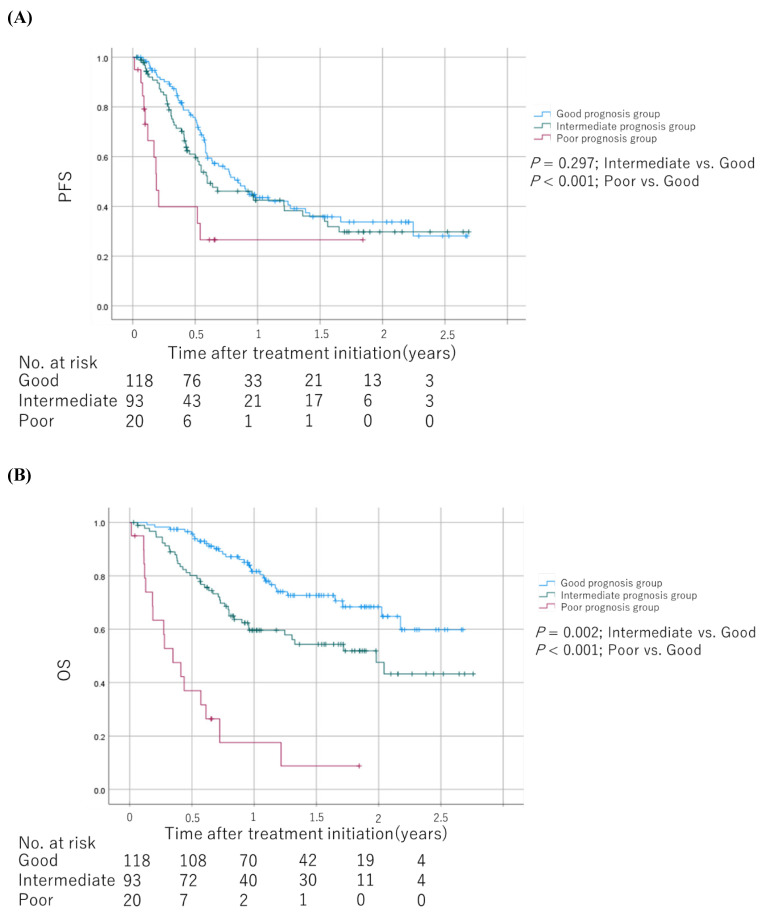
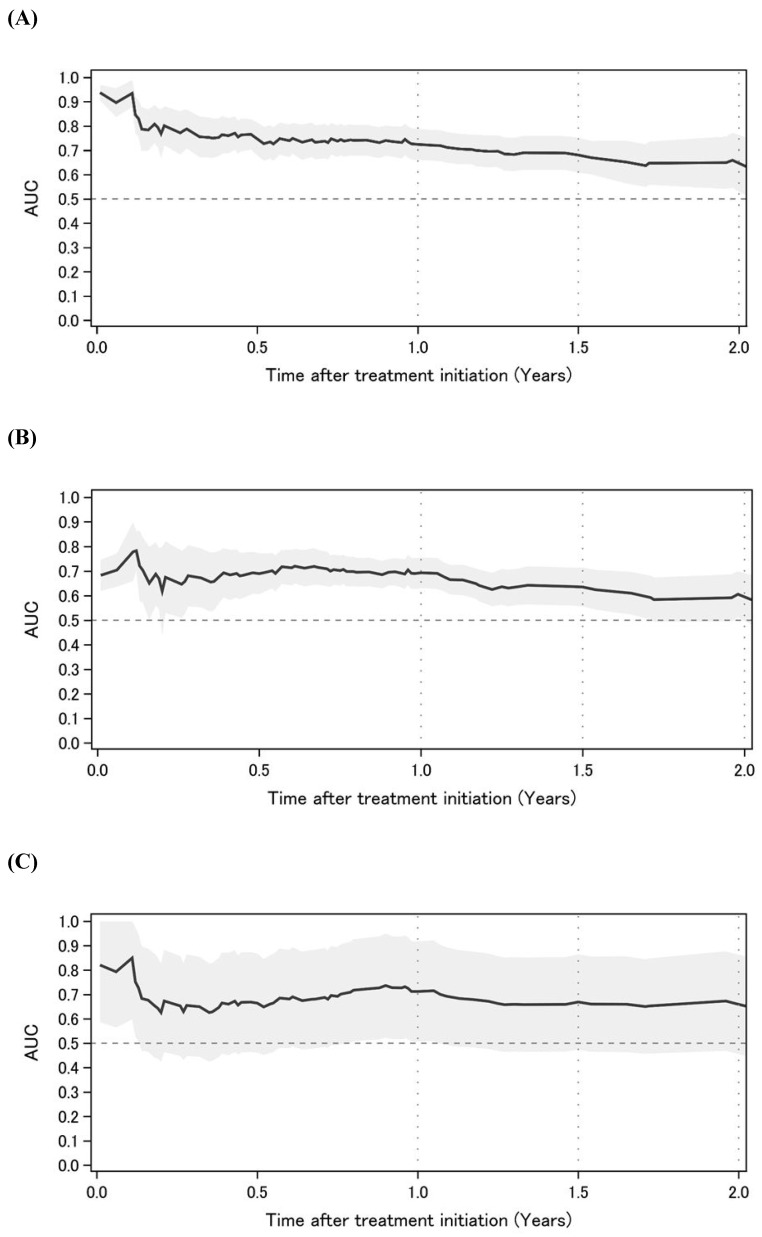
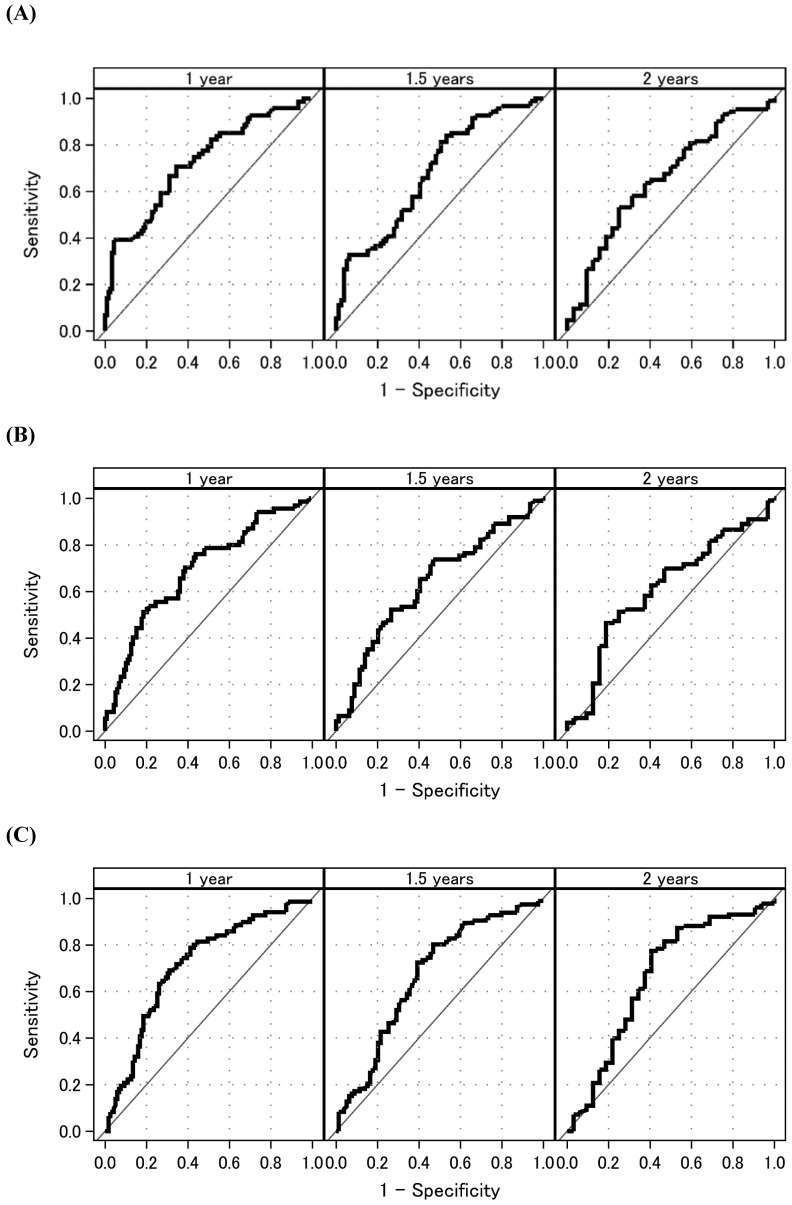
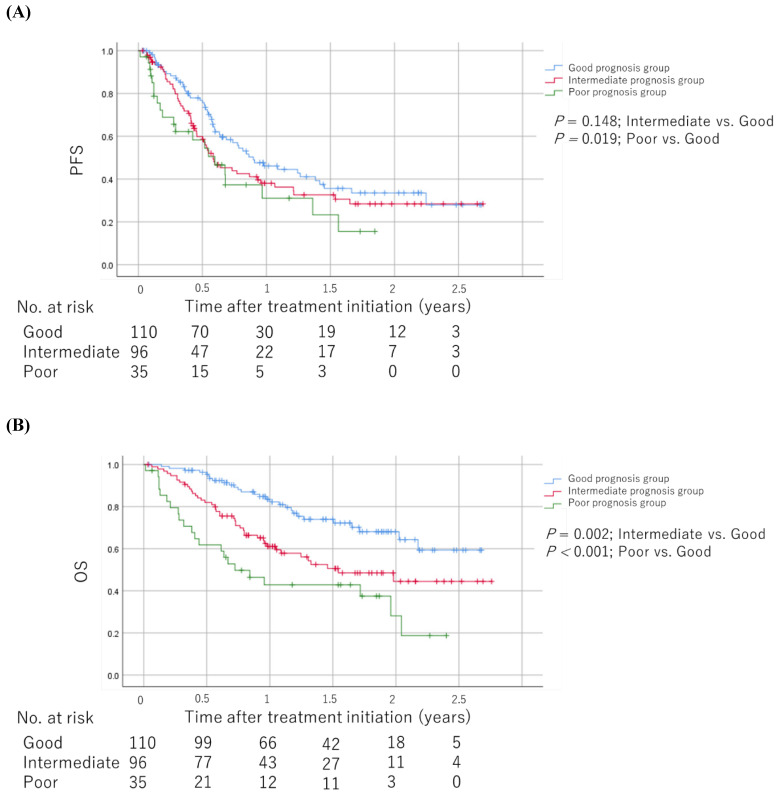
Association between baseline medications plus neutrophil-to-lymphocyte ratio (NLR) and the effectiveness of immune checkpoint inhibitor (ICI) plus platinum doublet remains unknown, despite several reported prognostic models. We used real-world data to investigate whether baseline medications plus NLR predict survival outcomes in patients with advanced non-small-cell lung cancer (NSCLC) receiving ICI plus platinum doublet. This multicenter, retrospective, observational study conducted in Japan between December 2018 and March 2021 used real-world data of consecutive patients with advanced NSCLC who received ICI (pembrolizumab or atezolizumab) plus platinum doublet as first-line treatment. Progression-free survival (PFS) and overall survival (OS) were estimated using the Kaplan-Meier method. The prognostic score for baseline medications plus NLR was weighted by regression β coefficients and used to categorize patients into good, intermediate, and poor prognoses groups. In addition, time-dependent receiver operating characteristic curve analyses and univariable and multivariable Cox proportional hazards models were constructed. Overall, 241 patients were included. Poor prognosis was significantly associated with worse PFS (hazard ratio [HR]: 1.78; 95% confidence interval [CI]: 1.08-2.94; = 0.025) and OS (HR: 3.59; 95% CI: 2.05-6.28; < 0.001) than good prognosis. Harrell's C-index for this prognostic model was 0.648. Baseline medication plus NLR could predict progressively worse survival outcomes in patients with advanced NSCLC receiving ICI plus platinum doublet and could be used as a prognostic index for poor outcomes.
尽管已有几种报道的预后模型,但基线用药加上中性粒细胞与淋巴细胞比值(NLR)与免疫检查点抑制剂(ICI)加铂类双联化疗的疗效之间的关联仍不清楚。我们使用真实世界数据来研究基线用药加上NLR是否能预测接受ICI加铂类双联化疗的晚期非小细胞肺癌(NSCLC)患者的生存结局。这项多中心、回顾性、观察性研究于2018年12月至2021年3月在日本进行,使用了连续接受ICI(帕博利珠单抗或阿替利珠单抗)加铂类双联化疗作为一线治疗的晚期NSCLC患者的真实世界数据。采用Kaplan-Meier法估计无进展生存期(PFS)和总生存期(OS)。基线用药加上NLR的预后评分通过回归β系数加权,并用于将患者分为预后良好、中等和不良组。此外,构建了时间依赖性受试者工作特征曲线分析以及单变量和多变量Cox比例风险模型。总体而言,纳入了241例患者。与预后良好相比,预后不良与更差的PFS(风险比[HR]:1.78;95%置信区间[CI]:1.08 - 2.94;P = 0.025)和OS(HR:3.59;95% CI:2.05 - 6.28;P < 0.001)显著相关。该预后模型的Harrell's C指数为0.648。基线用药加上NLR可以预测接受ICI加铂类双联化疗的晚期NSCLC患者生存结局逐渐变差,并可作为不良结局的预后指标。