Department of Surgery, Leiden University Medical Center (LUMC), Albinusdreef 2, Leiden, 2333 ZA, The Netherlands.
OncoStem Diagnostics Pvt Ltd, #4, Raja Ram Mohan Roy Road, Aanand Tower, 2nd Floor, Bangalore, 560027, India.
Breast Cancer Res. 2023 Apr 14;25(1):40. doi: 10.1186/s13058-023-01643-2.
Hormone receptor (HR)-positive, HER2/neu-negative breast cancers have a sustained risk of recurrence up to 20 years from diagnosis. TEAM (Tamoxifen, Exemestane Adjuvant Multinational) is a large, multi-country, phase III trial that randomized 9776 women for the use of hormonal therapy. Of these 2754 were Dutch patients. The current study aims for the first time to correlate the ten-year clinical outcomes with predictions by CanAssist Breast (CAB)-a prognostic test developed in South East Asia, on a Dutch sub-cohort that participated in the TEAM. The total Dutch TEAM cohort and the current Dutch sub-cohort were almost similar with respect to patient age and tumor anatomical features.
Of the 2754 patients from the Netherlands, which are part of the original TEAM trial, 592 patients' samples were available with Leiden University Medical Center (LUMC). The risk stratification of CAB was correlated with outcomes of patients using logistic regression approaches entailing Kaplan-Meier survival curves, univariate and multivariate cox-regression hazards model. We used hazard ratios (HRs), the cumulative incidence of distant metastasis/death due to breast cancer (DM), and distant recurrence-free interval (DRFi) for assessment.
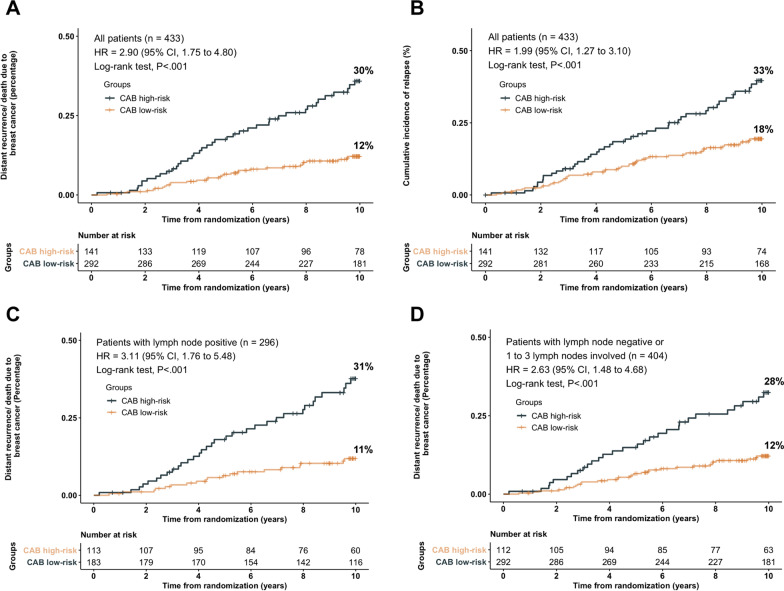
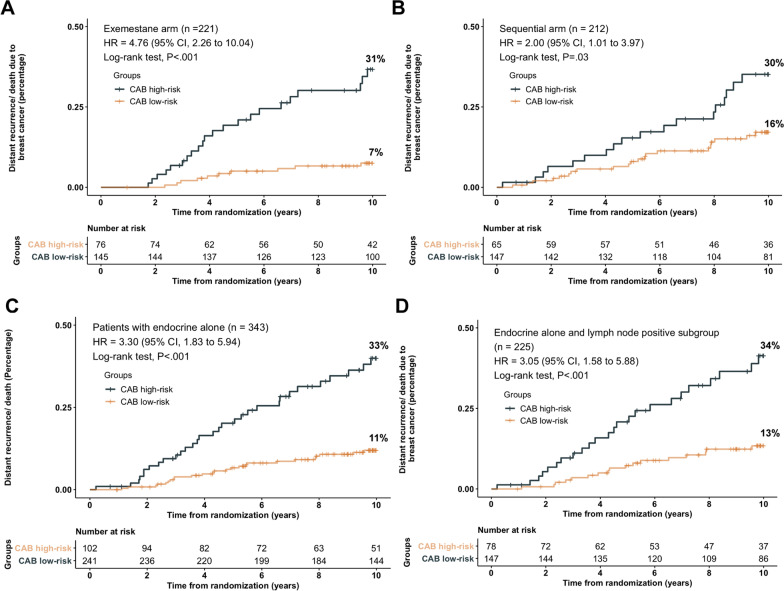
Out of 433 patients finally included, the majority, 68.4% had lymph node-positive disease, while only a minority received chemotherapy (20.8%) in addition to endocrine therapy. CAB stratified 67.5% of the total cohort as low-risk [DM = 11.5% (95% CI, 7.6-15.2)] and 32.5% as high-risk [DM = 30.2% (95% CI, 21.9-37.6)] with an HR of 2.90 (95% CI, 1.75-4.80; P < 0.001) at ten years. CAB risk score was an independent prognostic factor in the consideration of clinical parameters in multivariate analysis. At ten years, CAB high-risk had the worst DRFi of 69.8%, CAB low-risk in the exemestane monotherapy arm had the best DRFi of 92.7% [vs CAB high-risk, HR, 0.21 (95% CI, 0.11-0.43), P < 0.001], and CAB low-risk in the sequential arm had a DRFi of 84.2% [vs CAB high-risk, HR, 0.48 (95% CI, 0.28-0.82), P = 0.009].
Cost-effective CAB is a statistically robust prognostic and predictive tool for ten-year DM for postmenopausal women with HR+/HER2-, early breast cancer. CAB low-risk patients who received exemestane monotherapy had an excellent ten-year DRFi.
激素受体(HR)阳性、HER2/neu 阴性的乳腺癌在诊断后 20 年内仍有持续的复发风险。TEAM(他莫昔芬、依西美坦辅助多国)是一项大型的、多国家的 III 期试验,对 9776 名女性进行了激素治疗的随机分组。其中 2754 名是荷兰患者。目前的研究首次旨在通过 CanAssist Breast(CAB)——在东南亚开发的一种预后测试,与参与 TEAM 的荷兰亚组进行十年临床结果的相关性。荷兰 TEAM 队列的总人数和当前的荷兰亚组在患者年龄和肿瘤解剖特征方面几乎相似。
在荷兰的 2754 名来自原始 TEAM 试验的患者中,莱顿大学医学中心(LUMC)有 592 名患者的样本可用。CAB 的风险分层与使用逻辑回归方法的患者结果相关,包括 Kaplan-Meier 生存曲线、单变量和多变量 Cox 回归风险模型。我们使用风险比(HR)、远处转移/死于乳腺癌(DM)的累积发生率和远处无复发生存间隔(DRFi)进行评估。
在最终纳入的 433 名患者中,大多数患者(68.4%)患有淋巴结阳性疾病,只有少数患者(20.8%)除内分泌治疗外还接受了化疗。CAB 将总队列的 67.5%分层为低风险[DM=11.5%(95%CI,7.6-15.2)],32.5%为高风险[DM=30.2%(95%CI,21.9-37.6)],风险比(HR)为 2.90(95%CI,1.75-4.80;P<0.001)在十年。在多变量分析中,CAB 风险评分是临床参数考虑的独立预后因素。在十年时,CAB 高风险的 DRFi 最差,为 69.8%,CAB 低风险的依西美坦单药治疗组的 DRFi 最好,为 92.7%[与 CAB 高风险相比,HR 为 0.21(95%CI,0.11-0.43),P<0.001],而 CAB 低风险的序贯组的 DRFi 为 84.2%[与 CAB 高风险相比,HR 为 0.48(95%CI,0.28-0.82),P=0.009]。
具有成本效益的 CAB 是一种统计上稳健的预测和预测工具,可用于预测绝经后 HR+/HER2-、早期乳腺癌患者 10 年的 DM。接受依西美坦单药治疗的 CAB 低风险患者 10 年 DRFi 非常好。