Nicholson Andrew A, Densmore Maria, Frewen Paul A, Neufeld Richard W J, Théberge Jean, Jetly Rakesh, Lanius Ruth A, Ros Tomas
School of Psychology, University of Ottawa, Ottawa, Canada.
Atlas Institute for Veterans and Families, Royal Ottawa Hospital, Ottawa, Canada.
Brain Commun. 2023 Mar 16;5(2):fcad068. doi: 10.1093/braincomms/fcad068. eCollection 2023.
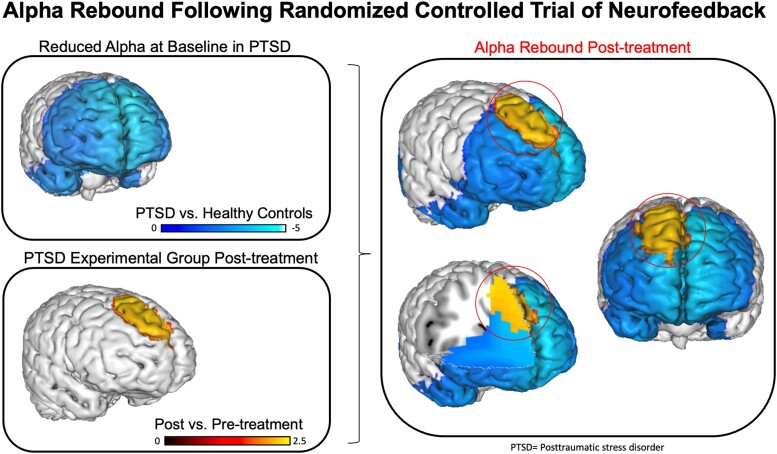
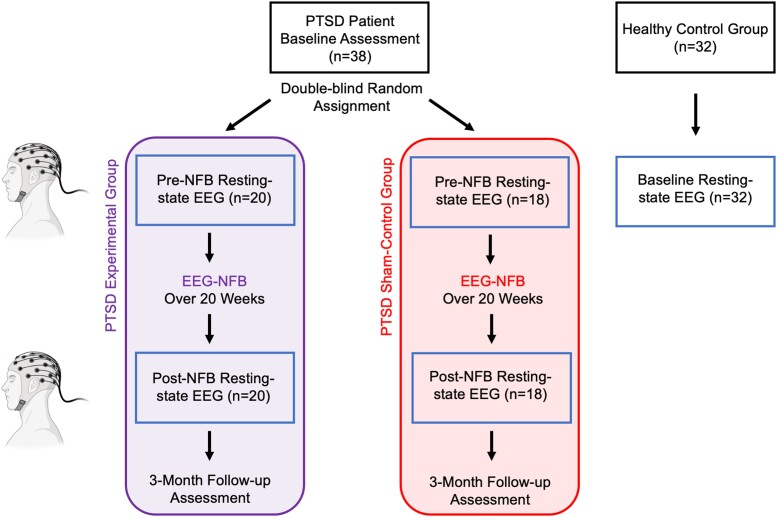
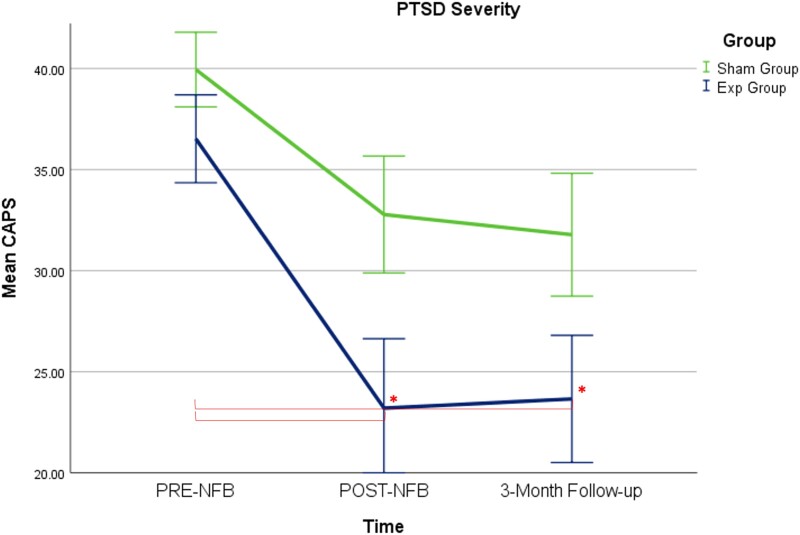
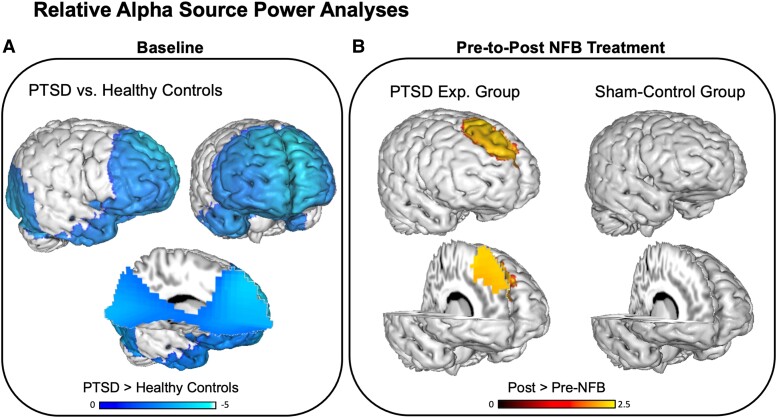
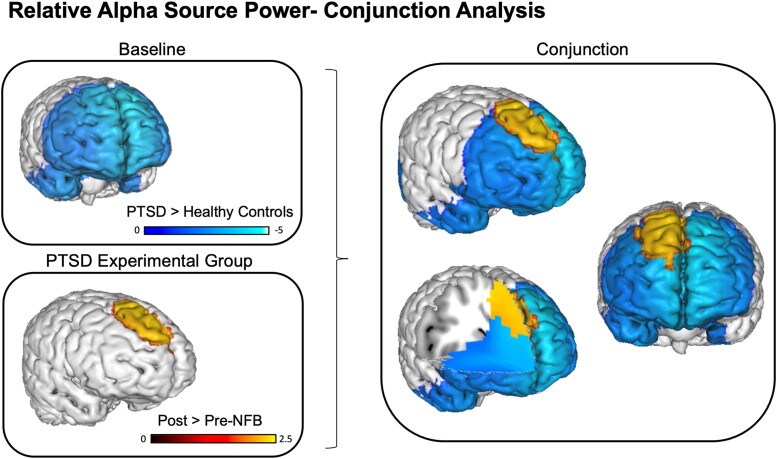
Collective research has identified a key electroencephalogram signature in patients with post-traumatic stress disorder, consisting of abnormally reduced alpha (8-12 Hz) rhythms. We conducted a 20-session, double-blind, randomized controlled trial of alpha desynchronizing neurofeedback in patients with post-traumatic stress disorder over 20 weeks. Our objective was to provide mechanistic evidence underlying potential clinical improvements by examining changes in aberrant post-traumatic stress disorder brain rhythms (namely, alpha oscillations) as a function of neurofeedback treatment. We randomly assigned participants with a primary diagnosis of post-traumatic stress disorder ( = 38) to either an experimental group ( = 20) or a sham-control group ( = 18). A multichannel electroencephalogram cap was used to record whole-scalp resting-state activity pre- and post-neurofeedback treatment, for both the experimental and sham-control post-traumatic stress disorder groups. We first observed significantly reduced relative alpha source power at baseline in patients with post-traumatic stress disorder as compared to an age/sex-matched group of neurotypical healthy controls ( = 32), primarily within regions of the anterior default mode network. Post-treatment, we found that only post-traumatic stress disorder patients in the experimental neurofeedback group demonstrated significant alpha resynchronization within areas that displayed abnormally low alpha power at baseline. In parallel, we observed significantly decreased post-traumatic stress disorder severity scores in the experimental neurofeedback group only, when comparing baseline to post-treatment (Cohen's = 0.77) and three-month follow-up scores (Cohen's = 0.75), with a remission rate of 60.0% at the three-month follow-up. Overall, our results indicate that neurofeedback training can rescue pathologically reduced alpha rhythmicity, a functional biomarker that has repeatedly been linked to symptoms of hyperarousal and cortical disinhibition in post-traumatic stress disorder. This randomized controlled trial provides long-term evidence suggesting that the 'alpha rebound effect' (i.e. homeostatic alpha resynchronization) occurs within key regions of the default mode network previously implicated in post-traumatic stress disorder.
集体研究已经确定了创伤后应激障碍患者的一种关键脑电图特征,其表现为α波(8-12赫兹)节律异常降低。我们针对创伤后应激障碍患者开展了一项为期20周、共20节次的双盲随机对照试验,采用α波去同步化神经反馈疗法。我们的目标是通过检查异常的创伤后应激障碍脑节律(即α波振荡)作为神经反馈治疗的函数的变化,为潜在的临床改善提供机制证据。我们将初步诊断为创伤后应激障碍的参与者(n = 38)随机分为实验组(n = 20)或假对照组(n = 18)。使用多通道脑电图帽记录实验组和假对照创伤后应激障碍组在神经反馈治疗前后的全脑静息状态活动。我们首先观察到,与年龄/性别匹配的神经典型健康对照组(n = 32)相比,创伤后应激障碍患者在基线时相对α波源功率显著降低,主要在前默认模式网络区域内。治疗后,我们发现只有实验组的创伤后应激障碍患者在基线时α波功率异常低的区域内表现出显著的α波重新同步化。同时,当比较基线与治疗后(科恩d = 0.77)以及三个月随访评分(科恩d = 0.75)时,我们仅在实验组观察到创伤后应激障碍严重程度评分显著降低,三个月随访时缓解率为60.0%。总体而言,我们的结果表明,神经反馈训练可以挽救病理性降低的α波节律,这是一种功能生物标志物,多次与创伤后应激障碍中的过度觉醒和皮层去抑制症状相关。这项随机对照试验提供了长期证据,表明“α波反弹效应”(即稳态α波重新同步化)发生在先前与创伤后应激障碍相关的默认模式网络的关键区域内。