Evidence-Based Practice Center (Murad, Hasan, Alsibai, Abbas, Wang), Mayo Clinic, Rochester, Minn.; Department of Epidemiology and Biostatistics (Lin), University of Arizona, Tucson, Ariz.; Statistical Research and Data Science Center (Chu), Pfizer, New York, NY; Department of Internal Medicine (Mustafa), University of Kansas Health System, Kansas City, Kan.
CMAJ. 2023 Jul 17;195(27):E925-E931. doi: 10.1503/cmaj.221802.
Sensitivity and specificity are characteristics of a diagnostic test and are not expected to change as the prevalence of the target condition changes. We sought to evaluate the association between prevalence and changes in sensitivity and specificity.
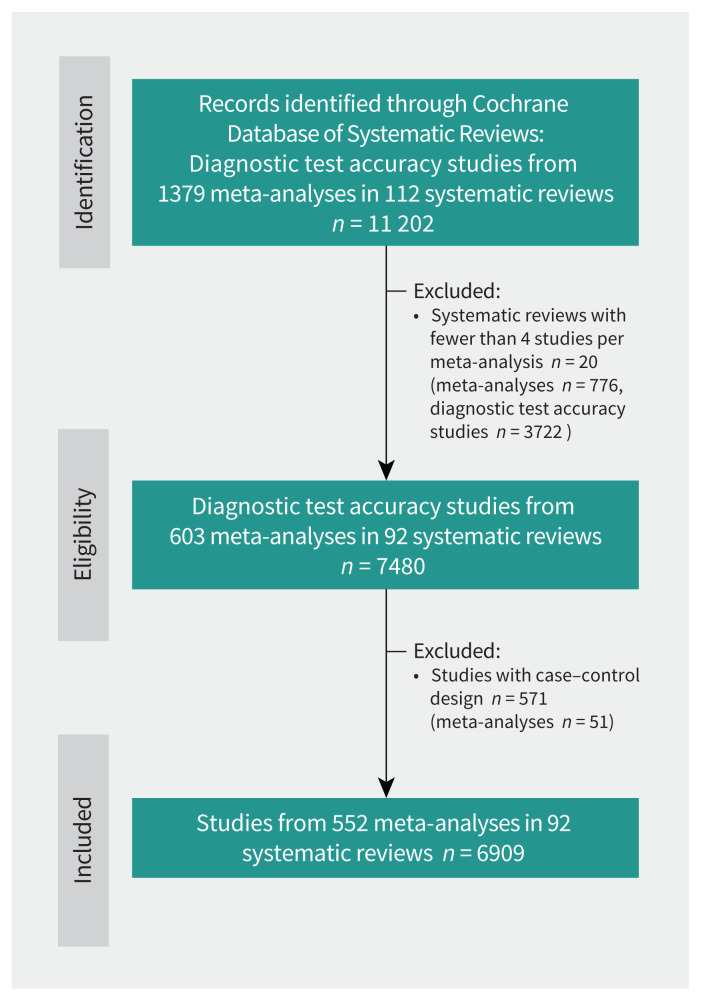
We retrieved data from meta-analyses of diagnostic test accuracy published in the Cochrane Database of Systematic Reviews (2003-2020). We used mixed-effects random-intercept linear regression models to evaluate the association between prevalence and logit-transformed sensitivity and specificity. The model evaluated all meta-analyses as nested within each systematic review.
We analyzed 6909 diagnostic test accuracy studies from 552 meta-analyses that were included in 92 systematic reviews. For sensitivity, compared with the lowest quartile of prevalence, the second, third and fourth quartiles were associated with significantly higher odds of identifying a true positive case (odds ratio [OR] 1.17, 95% confidence interval [CI] 1.09-1.26; OR 1.32, 95% CI 1.23-1.41; OR 1.47, 95% CI 1.37-1.58; respectively). For specificity, compared with the lowest quartile of prevalence, the second, third and fourth quartiles were associated with significantly lower odds of identifying a true negative case (OR 0.74, 95% CI 0.69-0.80; OR 0.65, 95% CI 0.60-0.70; OR 0.47, 95% CI 0.44-0.51; respectively). Pooled regression coefficients from bivariate models conducted within each meta-analysis showed that prevalence was positively associated with sensitivity and negatively associated with specificity. Findings were consistent across subgroups.
In this large sample of diagnostic studies, higher prevalence was associated with higher estimated sensitivity and lower estimated specificity. Clinicians should consider the implications of disease prevalence and spectrum when interpreting the results from studies of diagnostic test accuracy.
敏感性和特异性是诊断测试的特征,不应随着目标疾病的患病率变化而改变。我们旨在评估患病率与敏感性和特异性变化之间的关联。
我们从 Cochrane 系统评价数据库(2003-2020 年)发表的诊断准确性的荟萃分析中检索数据。我们使用混合效应随机截距线性回归模型评估患病率与对数转换敏感性和特异性之间的关联。该模型在每个系统评价内评估所有荟萃分析作为嵌套分析。
我们分析了来自 552 项荟萃分析的 6909 项诊断准确性研究,这些研究被纳入 92 项系统评价中。对于敏感性,与最低四分位数的患病率相比,第二、第三和第四四分位数与更高的识别真正阳性病例的几率显著相关(比值比 [OR] 1.17,95%置信区间 [CI] 1.09-1.26;OR 1.32,95%CI 1.23-1.41;OR 1.47,95%CI 1.37-1.58;分别)。对于特异性,与最低四分位数的患病率相比,第二、第三和第四四分位数与识别真正阴性病例的几率显著降低相关(OR 0.74,95%CI 0.69-0.80;OR 0.65,95%CI 0.60-0.70;OR 0.47,95%CI 0.44-0.51;分别)。在每个荟萃分析内进行的二元模型的汇总回归系数显示,患病率与敏感性呈正相关,与特异性呈负相关。亚组分析结果一致。
在这项大型诊断研究样本中,较高的患病率与较高的估计敏感性和较低的估计特异性相关。临床医生在解释诊断测试准确性研究的结果时,应考虑疾病患病率和谱的影响。