Department of Medicine, Laboratory of Molecular Medicine and Biotechnology, University Campus Bio-Medico of Rome, Rome, Italy.
Institute of Translational Pharmacology, National Research Council of Italy (CNR), Rome, Italy.
J Exp Clin Cancer Res. 2023 Jul 17;42(1):170. doi: 10.1186/s13046-023-02754-6.
Approximately 20-50% of patients presenting with localized colorectal cancer progress to stage IV metastatic disease (mCRC) following initial treatment and this is a major prognostic determinant. Here, we have interrogated a heterogeneous set of primary colorectal cancer (CRC), liver CRC metastases and adjacent liver tissue to identify molecular determinants of the colon to liver spreading. Screening Food and Drug Administration (FDA) approved drugs for their ability to interfere with an identified colon to liver metastasis signature may help filling an unmet therapeutic need.
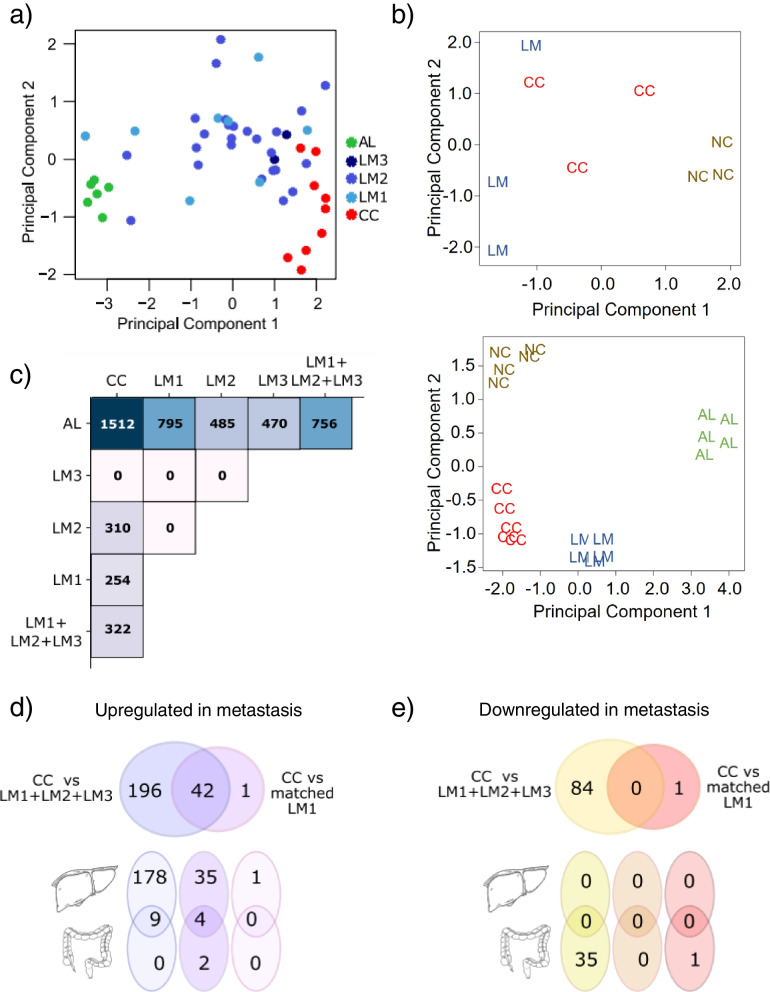
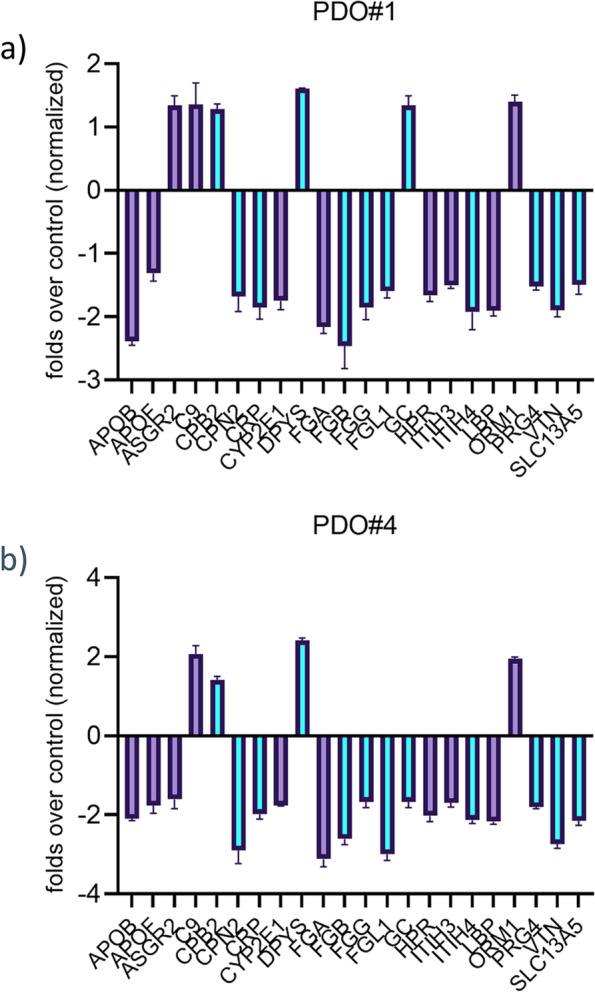
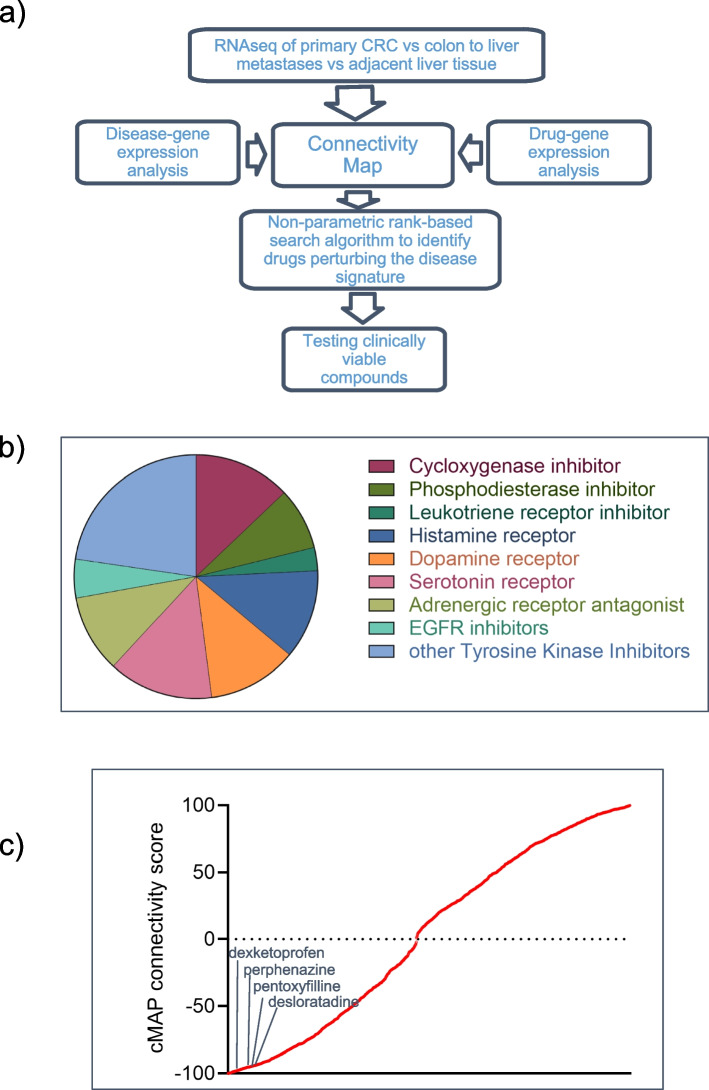
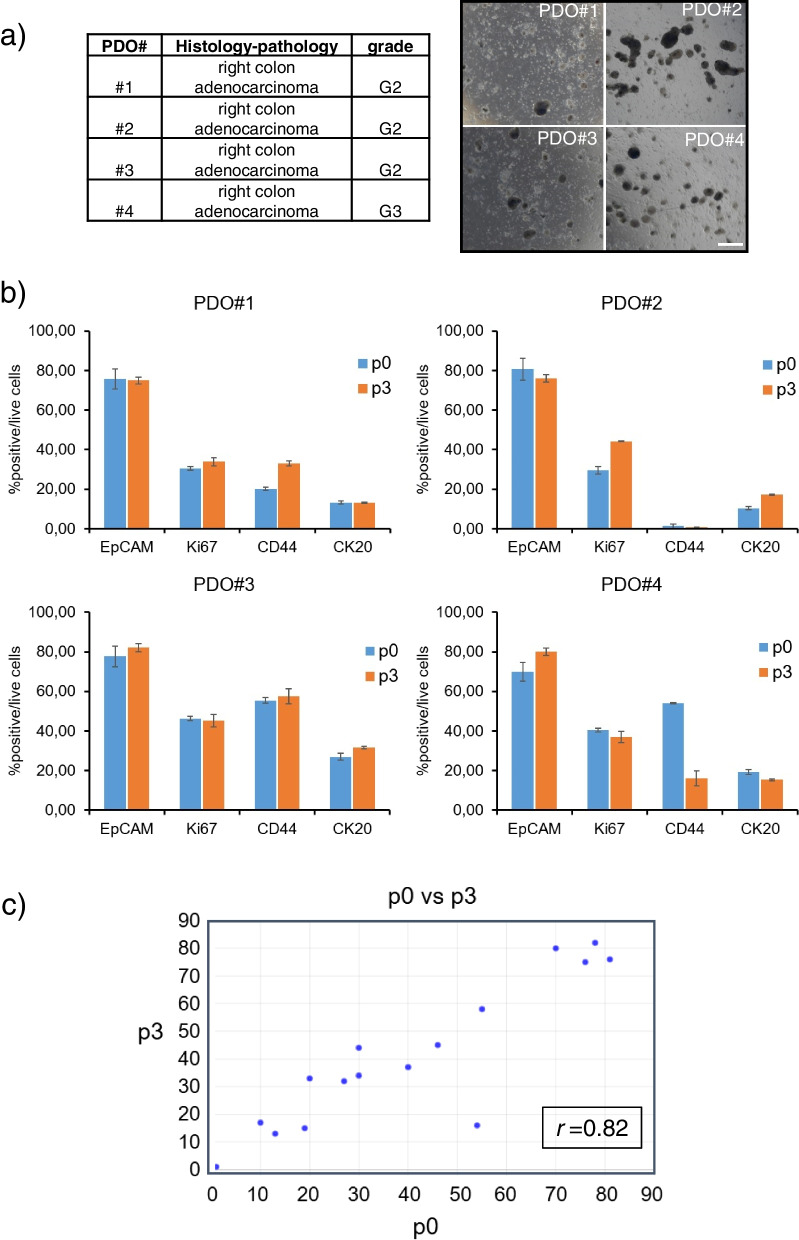
RNA sequencing of primary colorectal cancer specimens vs adjacent liver tissue vs synchronous and asynchronous liver metastases. Pathways enrichment analyses. The Library of Integrated Network-based Cellular Signatures (LINCS)-based and Connectivity Map (CMAP)-mediated identification of FDA-approved compounds capable to interfere with a 22 gene signature from primary CRC and liver metastases. Testing the identified compounds on CRC-Patient Derived Organoid (PDO) cultures. Microscopy and Fluorescence Activated Cell Sorting (FACS) based analysis of the treated PDOs.
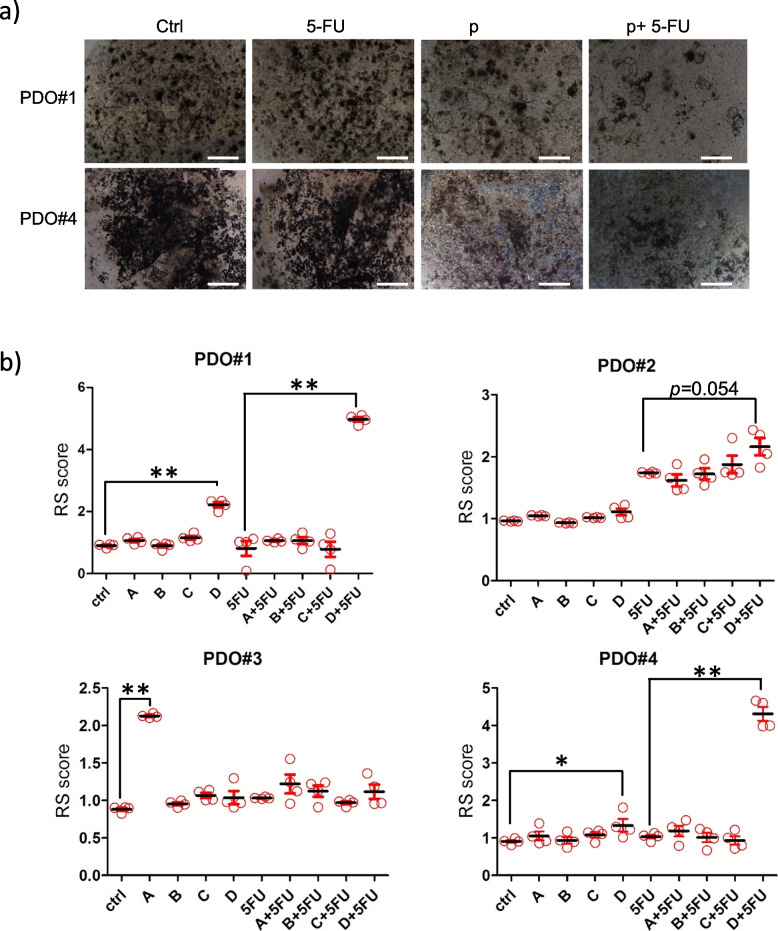
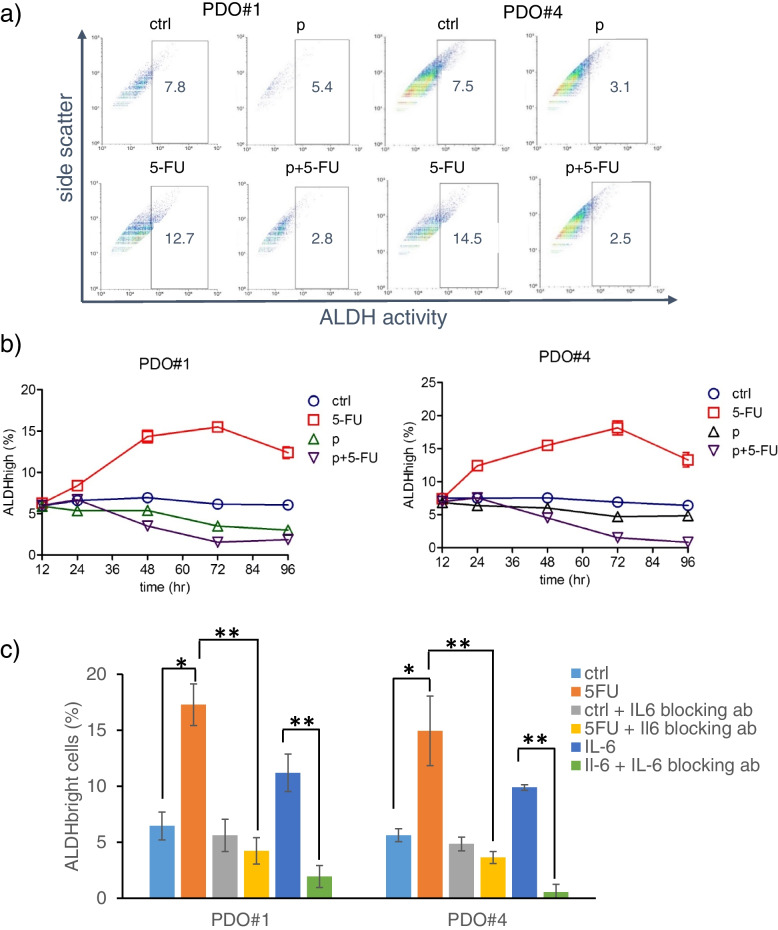
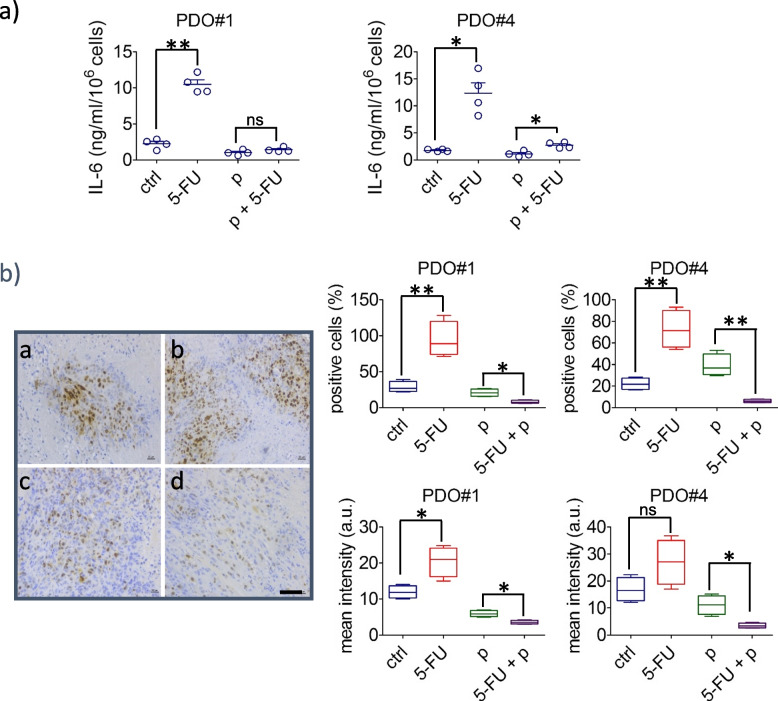
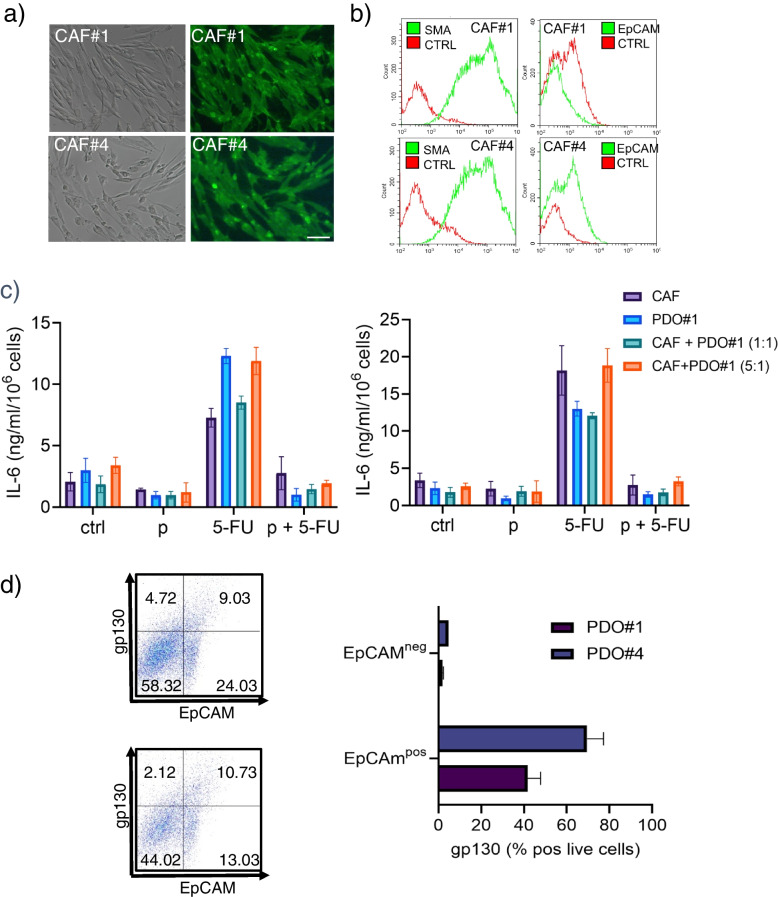
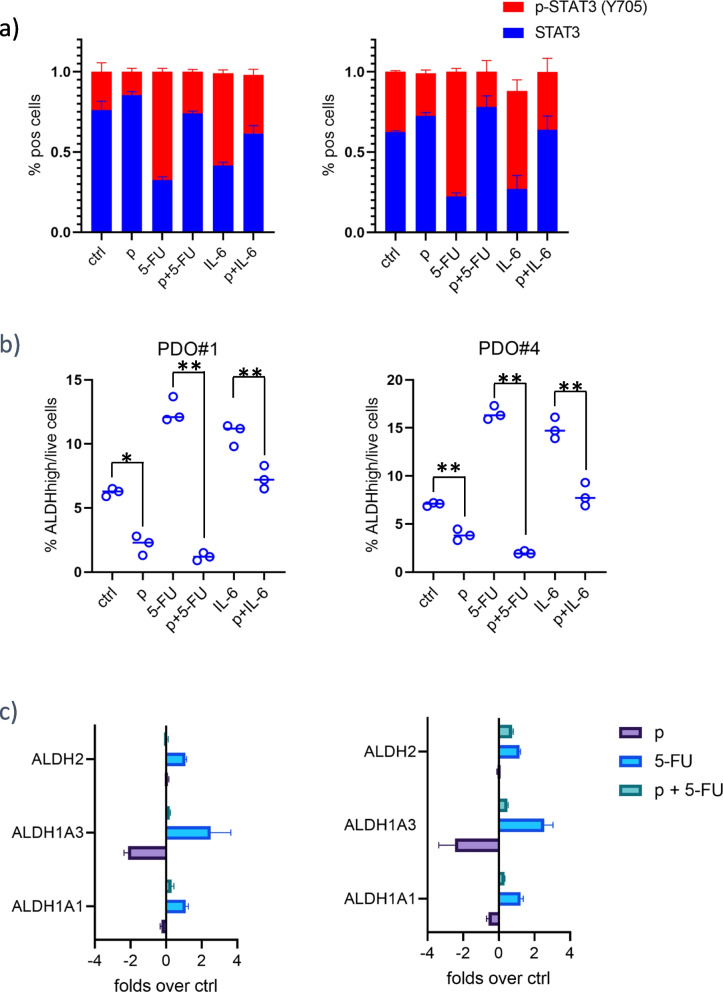
We have found that liver metastases acquire features of the adjacent liver tissue while partially losing those of the primary tumors they derived from. We have identified a 22-gene signature differentially expressed among primary tumors and metastases and validated in public databases. A pharmacogenomic screening for FDA-approved compounds capable of interfering with this signature has been performed. We have validated some of the identified representative compounds in CRC-Patient Derived Organoid cultures (PDOs) and found that pentoxyfilline and, to a minor extent, dexketoprofen and desloratadine, can variably interfere with number, size and viability of the CRC -PDOs in a patient-specific way. We explored the pentoxifylline mechanism of action and found that pentoxifylline treatment attenuated the 5-FU elicited increase of ALDHhigh cells by attenuating the IL-6 mediated STAT3 (tyr705) phosphorylation.
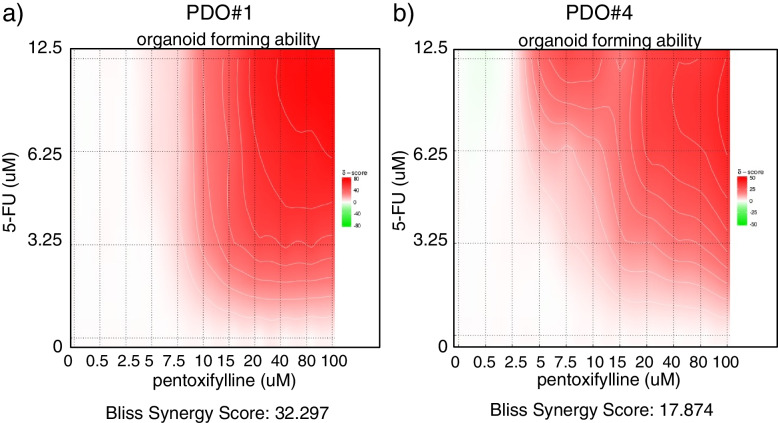
Pentoxifylline synergizes with 5-Fluorouracil (5-FU) in attenuating organoid formation. It does so by interfering with an IL-6-STAT3 axis leading to the emergence of chemoresistant ALDHhigh cell subpopulations in 5-FU treated PDOs. A larger cohort of CRC-PDOs will be required to validate and expand on the findings of this proof-of-concept study.
大约 20-50%局部结直肠癌患者在初始治疗后进展为 IV 期转移性疾病(mCRC),这是一个主要的预后决定因素。在这里,我们对一组异质的原发性结直肠癌(CRC)、肝 CRC 转移灶和相邻肝组织进行了研究,以确定向肝转移的分子决定因素。筛选食品和药物管理局(FDA)批准的药物以确定其是否能够干扰已确定的向肝转移特征,这可能有助于满足未满足的治疗需求。
对原发性结直肠癌标本与相邻肝组织、同步和异步肝转移灶进行 RNA 测序。通路富集分析。基于 LINCS(集成网络细胞特征文库)和 CMAP(连接图谱)的筛选,确定 FDA 批准的化合物能够干扰原发性 CRC 和肝转移灶的 22 个基因特征。在 CRC-患者衍生类器官(PDO)培养物上测试鉴定的化合物。对经处理的 PDO 进行显微镜和荧光激活细胞分选(FACS)分析。
我们发现,肝转移灶获得了相邻肝组织的特征,同时部分保留了其起源的原发性肿瘤的特征。我们确定了一组在原发性肿瘤和转移灶中差异表达的 22 个基因特征,并在公共数据库中进行了验证。对能够干扰该特征的 FDA 批准化合物进行了药物基因组筛选。我们在 CRC-患者衍生类器官(PDO)培养物中验证了一些鉴定出的代表性化合物,发现戊四醇和(程度较小)酮咯酸和地氯雷他定可在一定程度上以患者特异性方式改变 CRC-PDO 的数量、大小和活力。我们探讨了戊四醇的作用机制,发现戊四醇治疗通过减弱 IL-6 介导的 STAT3(tyr705)磷酸化,减弱了 5-FU 引起的 ALDHhigh 细胞的增加,从而减弱了类器官的形成。
戊四醇与 5-氟尿嘧啶(5-FU)协同作用,减弱类器官的形成。它通过干扰 IL-6-STAT3 轴,导致在 5-FU 处理的 PDO 中出现化学抗性 ALDHhigh 细胞亚群。需要更大的 CRC-PDO 队列来验证和扩展这项概念验证研究的结果。