Litwin Tomasz, Antos Agnieszka, Bembenek Jan, Przybyłkowski Adam, Kurkowska-Jastrzębska Iwona, Skowrońska Marta, Członkowska Anna
Second Department of Neurology, Institute of Psychiatry and Neurology, 02-957 Warsaw, Poland.
Department of Clinical Neurophysiology, Institute of Psychiatry and Neurology, 02-957 Warsaw, Poland.
Diagnostics (Basel). 2023 Jul 20;13(14):2424. doi: 10.3390/diagnostics13142424.
Treatment of Wilson's disease (WD), an inherited disease characterized by copper overload, is lifelong and there is the possibility that copper deficiency (CD) may occur. We systematically reviewed the literature to describe treatment patterns, symptoms and outcomes associated with CD.
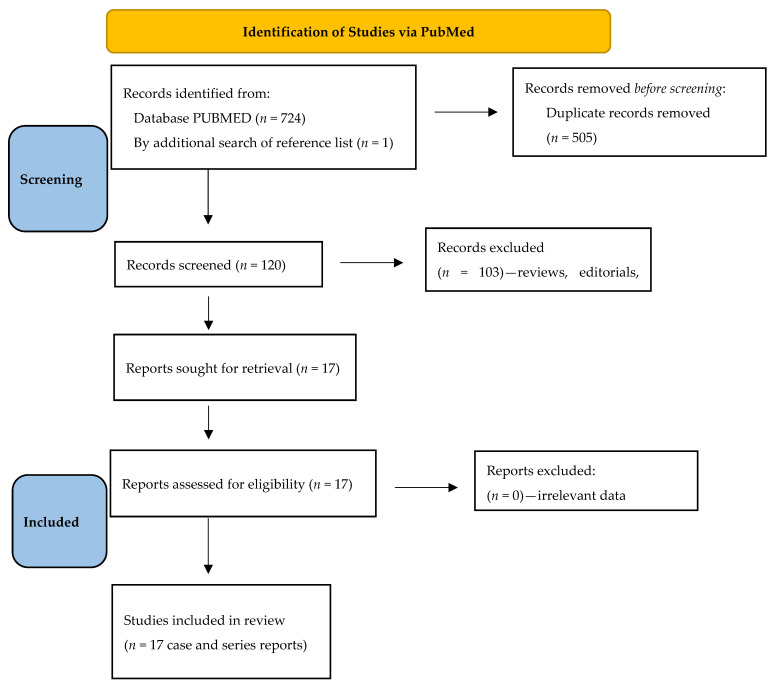
Using preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines, the PubMed database was searched up to 6 April 2023.
Across 17 articles, 20 cases of CD were described, most commonly (15 cases) in WD patients treated with zinc salts (ZS), less often on combined chelator and ZS therapy (3 cases), molybdate salts plus ZS (1), or molybdate alone (1). CD symptoms occurred insidiously, including sideroblastic anemia, neutropenia, axonal sensory neuropathy, posterior cord myelopathy and increased ratio of epileptic seizures (or epilepsy). CD diagnosis was based on symptoms and severely reduced urinary copper excretion (<20 µg/24 h [<0.3 µmol/24 h] on ZS, or <100 µg/24 h [<1.6 µmol/24 h] on chelators) with low total serum copper and ceruloplasmin.
Awareness of CD and regular monitoring of copper metabolism is needed during WD treatment. Temporary cessation of anti-copper treatment usually reverses serum copper reductions as well as pancytopenia; however, some symptoms, especially neuropathy and myelopathy, may persist.
威尔逊病(WD)是一种以铜过载为特征的遗传性疾病,其治疗是终身的,并且有可能发生铜缺乏(CD)。我们系统地回顾了文献,以描述与CD相关的治疗模式、症状和结局。
按照系统评价和Meta分析的首选报告项目(PRISMA)指南,检索PubMed数据库至2023年4月6日。
在17篇文章中,共描述了20例CD病例,最常见的(15例)是接受锌盐(ZS)治疗的WD患者,较少见的是联合螯合剂和ZS治疗(3例)、钼酸盐加ZS治疗(1例)或单独使用钼酸盐治疗(1例)。CD症状隐匿出现,包括铁粒幼细胞性贫血、中性粒细胞减少、轴索性感觉神经病、脊髓后索病变以及癫痫发作(或癫痫)比例增加。CD的诊断基于症状以及尿铜排泄严重减少(接受ZS治疗时<20μg/24小时[<0.3μmol/24小时],或接受螯合剂治疗时<100μg/24小时[<1.6μmol/24小时]),同时伴有血清总铜和铜蓝蛋白降低。
WD治疗期间需要认识到CD并定期监测铜代谢。暂时停止抗铜治疗通常可逆转血清铜降低以及全血细胞减少;然而,一些症状,尤其是神经病和脊髓病,可能会持续存在。