Lancet. 2023 Sep 23;402(10407):1065-1082. doi: 10.1016/S0140-6736(23)01088-7. Epub 2023 Aug 3.
Large disparities in mortality exist across racial-ethnic groups and by location in the USA, but the extent to which racial-ethnic disparities vary by location, or how these patterns vary by cause of death, is not well understood. We aimed to estimate age-standardised mortality by racial-ethnic group, county, and cause of death and describe the intersection between racial-ethnic and place-based disparities in mortality in the USA, comparing patterns across health conditions.
We applied small-area estimation models to death certificate data from the US National Vital Statistics system and population data from the US National Center for Health Statistics to estimate mortality by age, sex, county, and racial-ethnic group annually from 2000 to 2019 for 19 broad causes of death. Race and ethnicity were categorised as non-Latino and non-Hispanic American Indian or Alaska Native (AIAN), non-Latino and non-Hispanic Asian or Pacific Islander (Asian), non-Latino and non-Hispanic Black (Black), Latino or Hispanic (Latino), and non-Latino and non-Hispanic White (White). We adjusted these mortality rates to correct for misreporting of race and ethnicity on death certificates and generated age-standardised results using direct standardisation to the 2010 US census population.
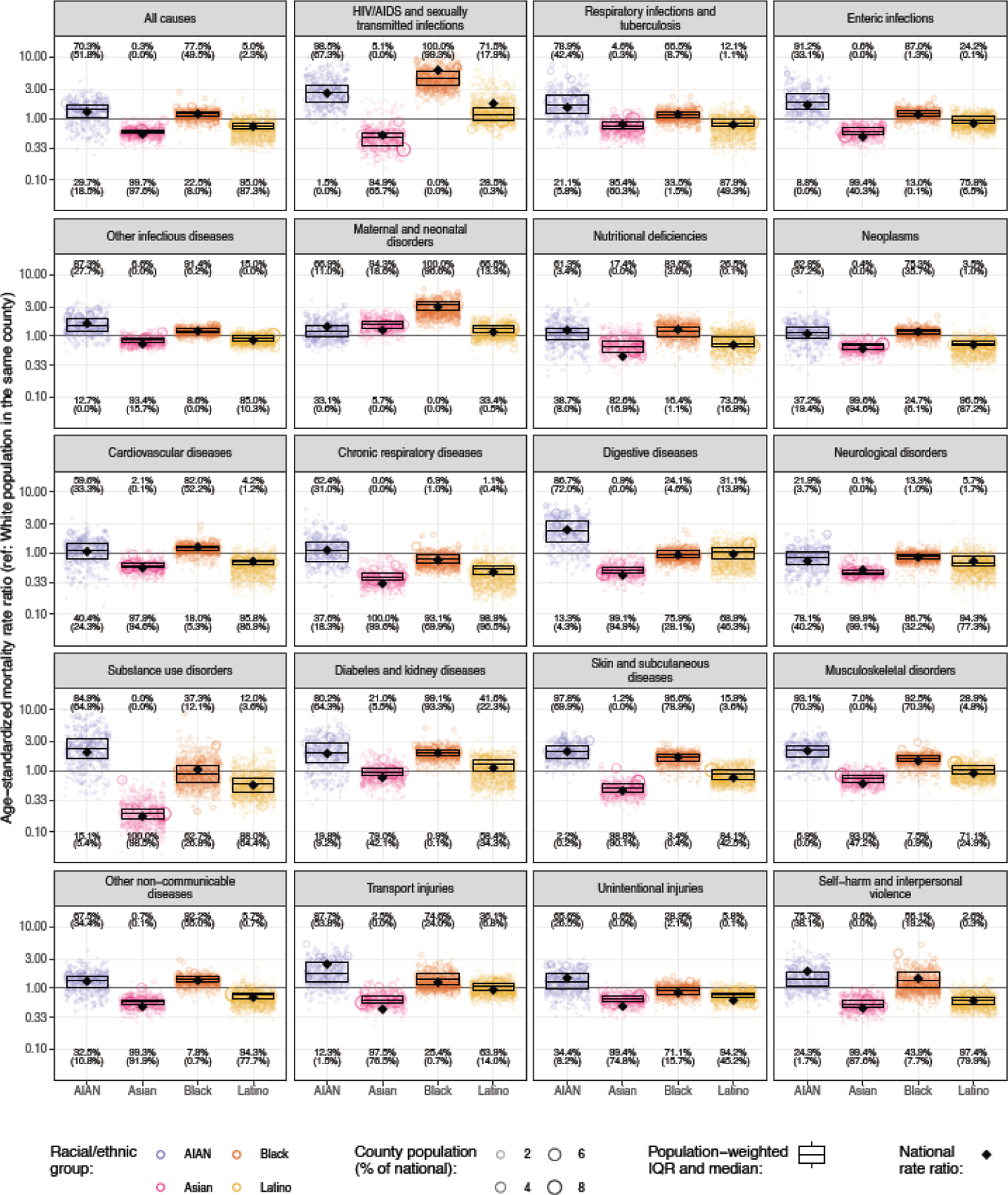
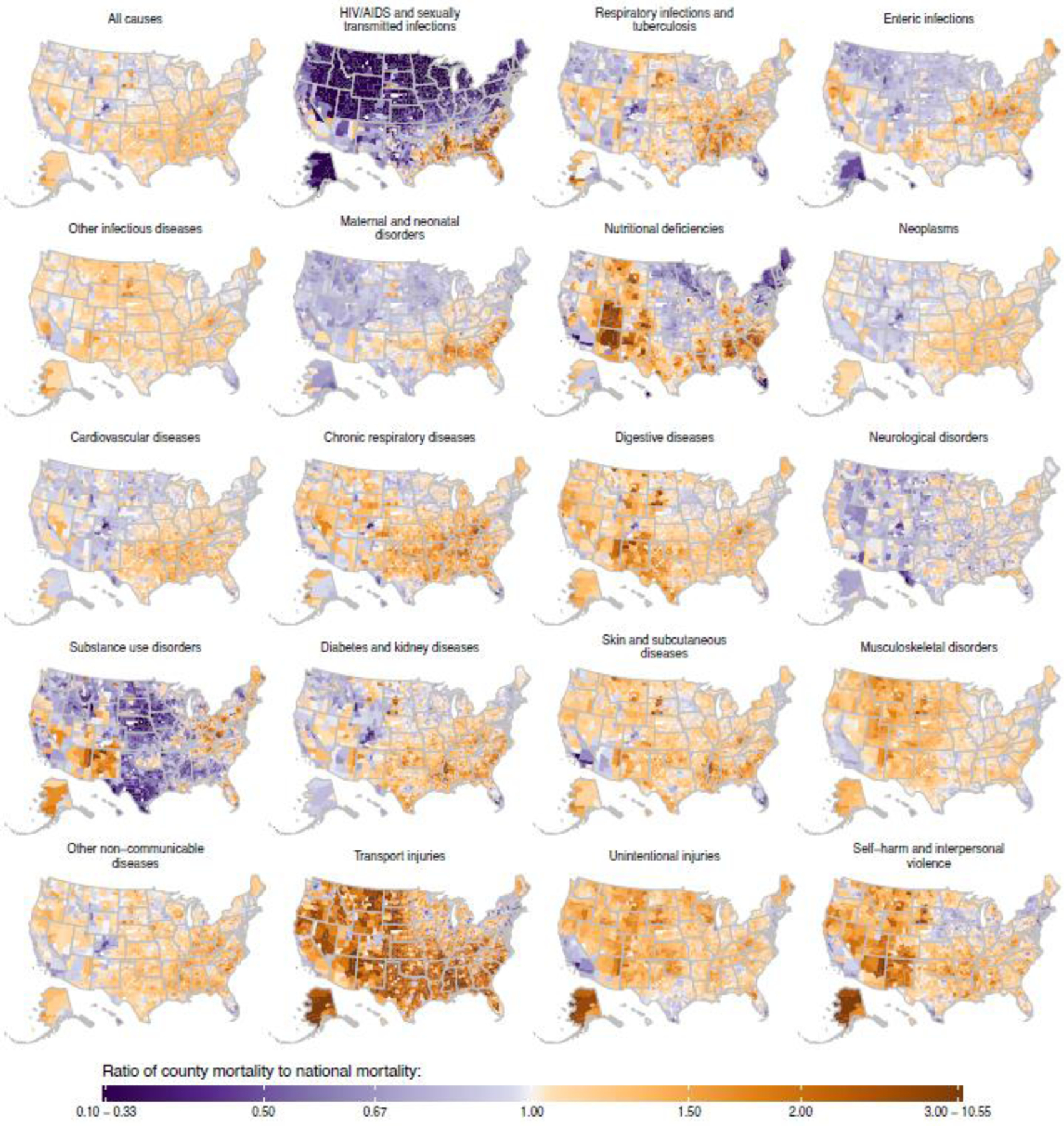
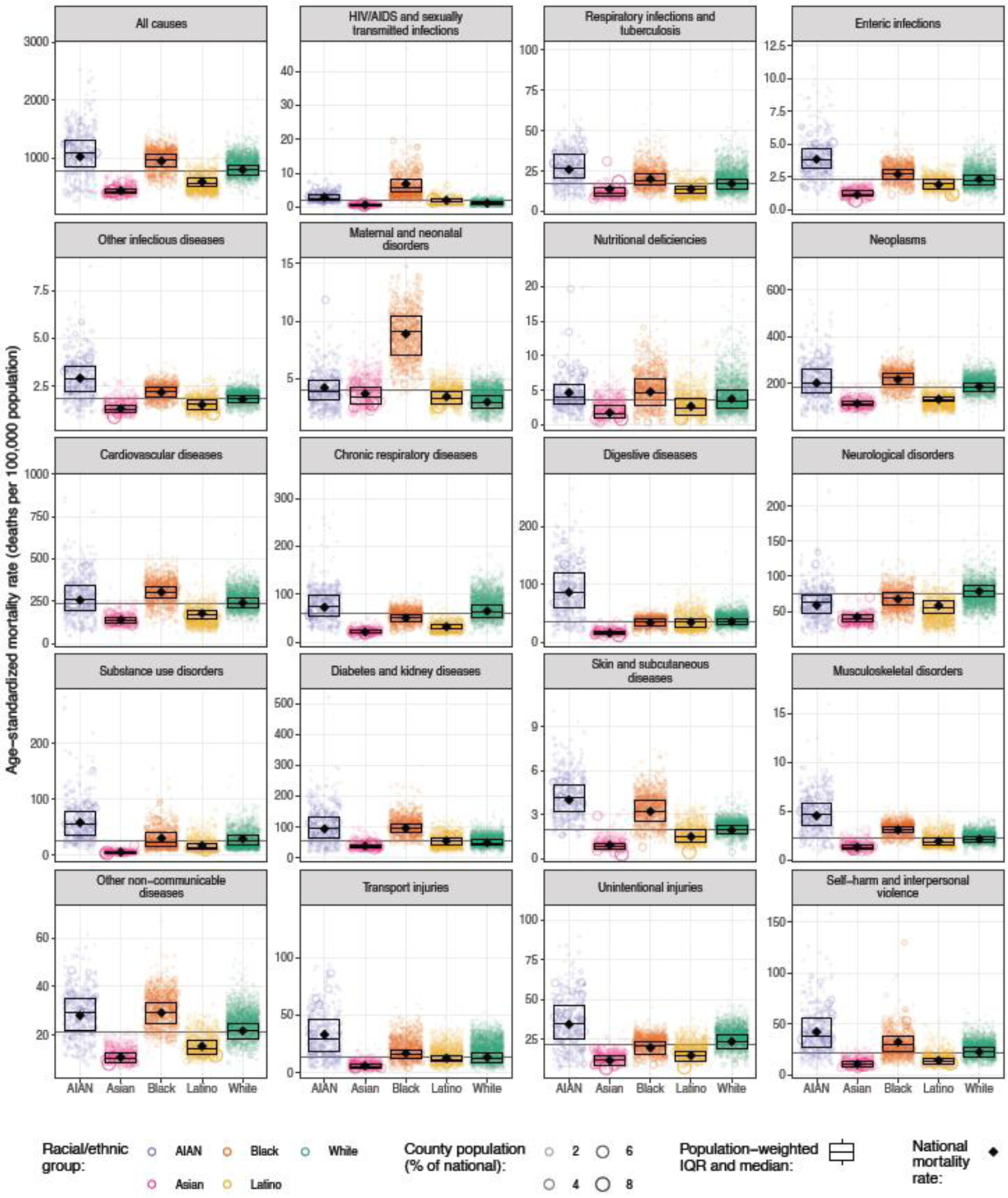
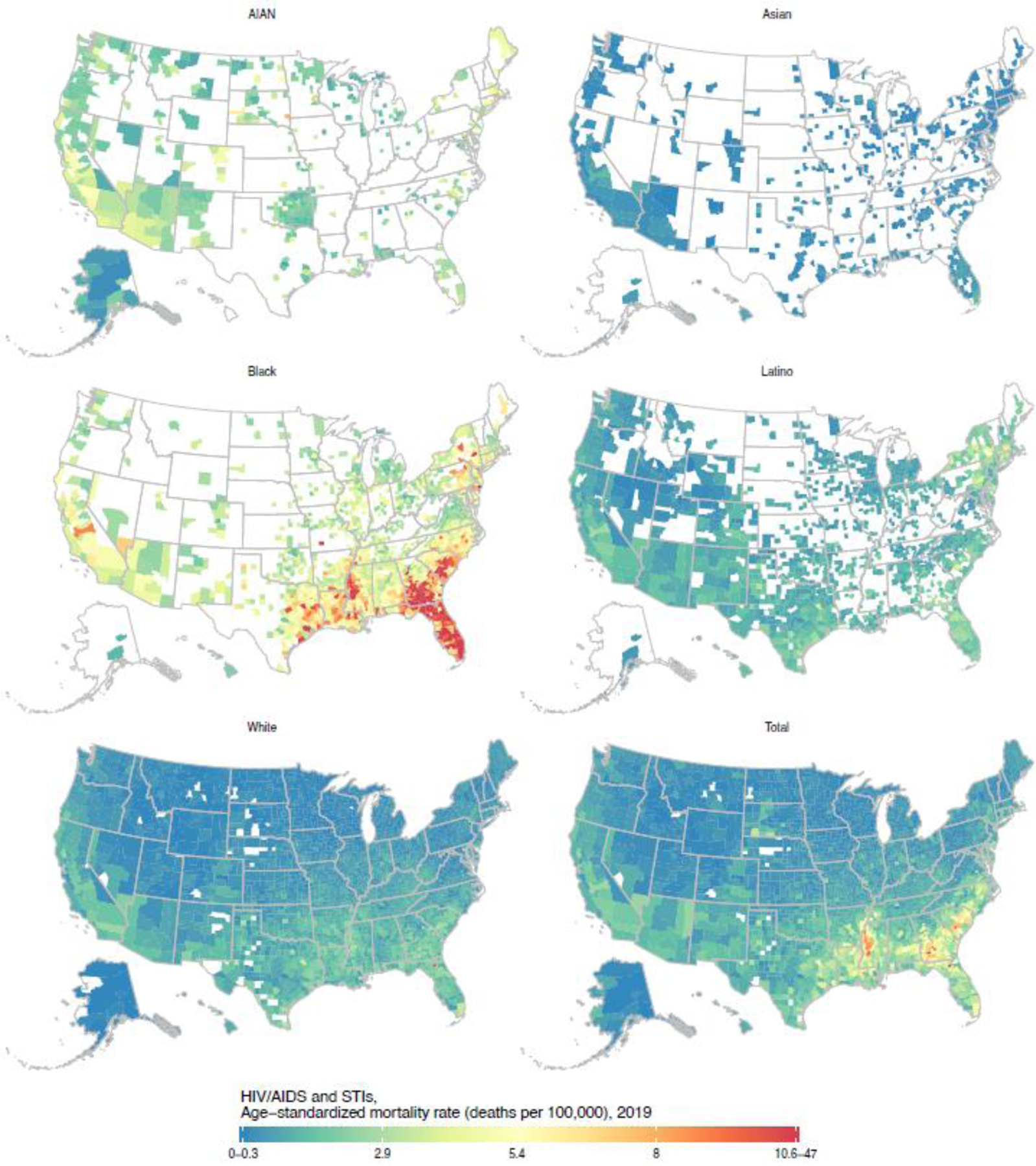
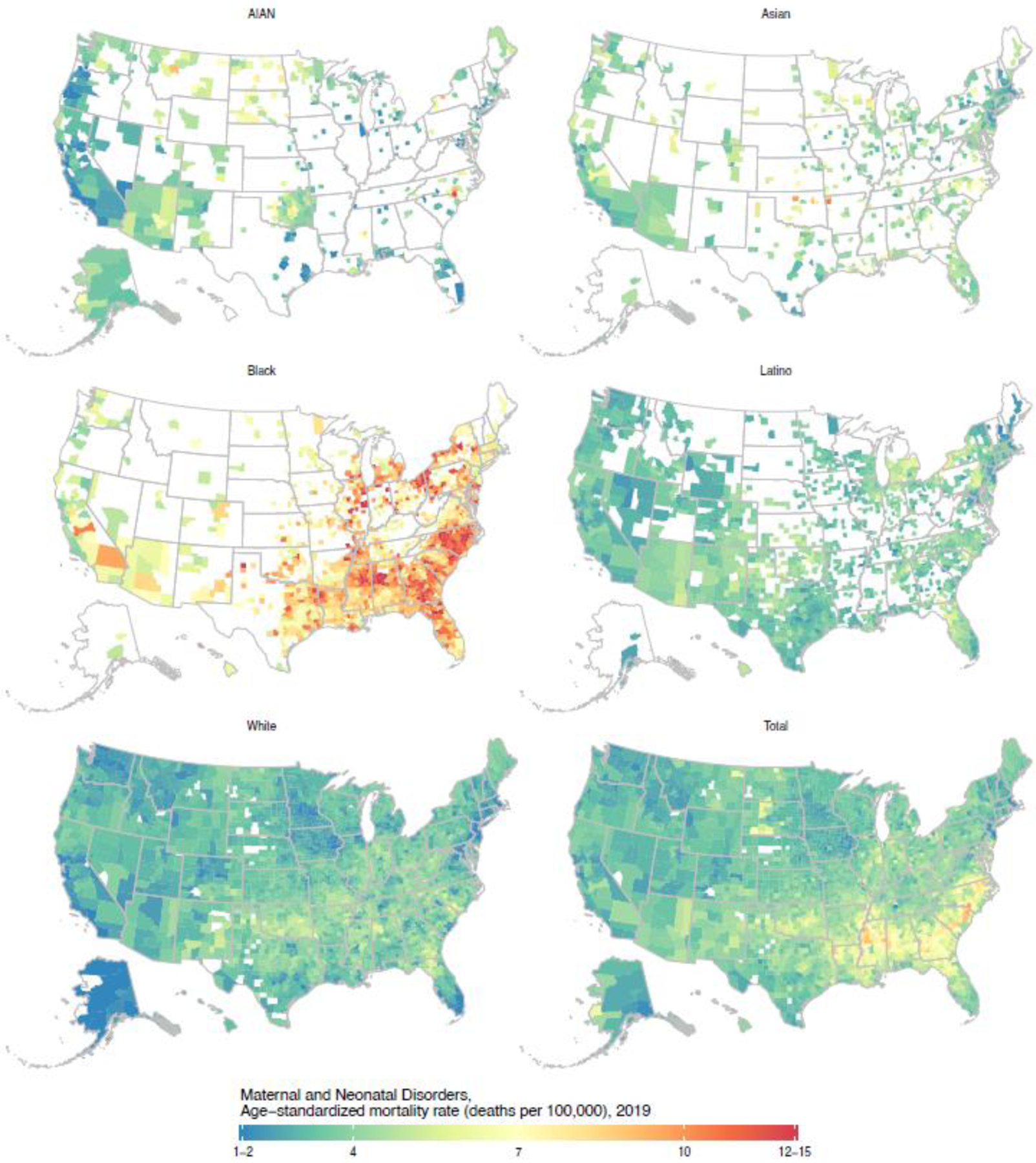
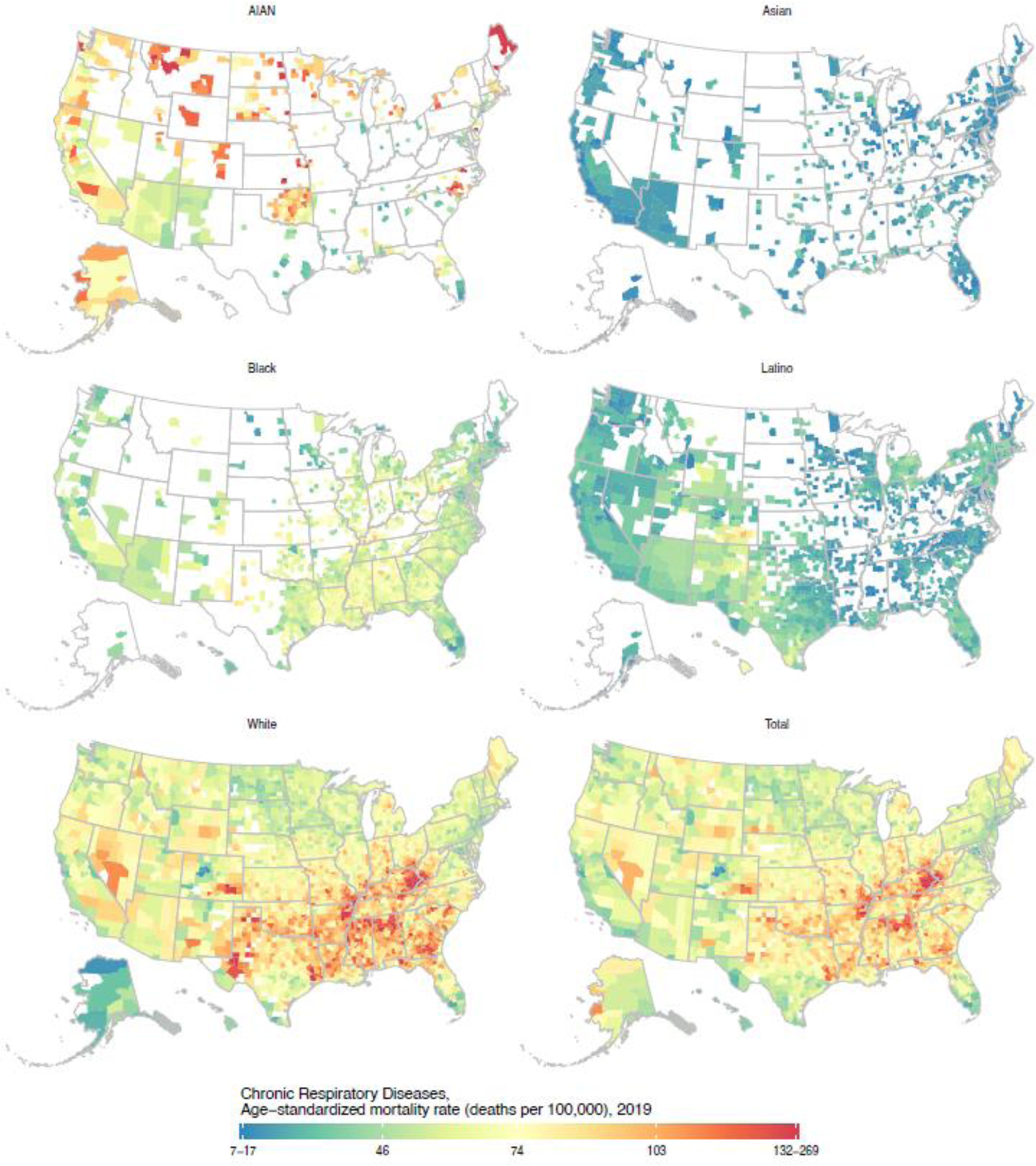
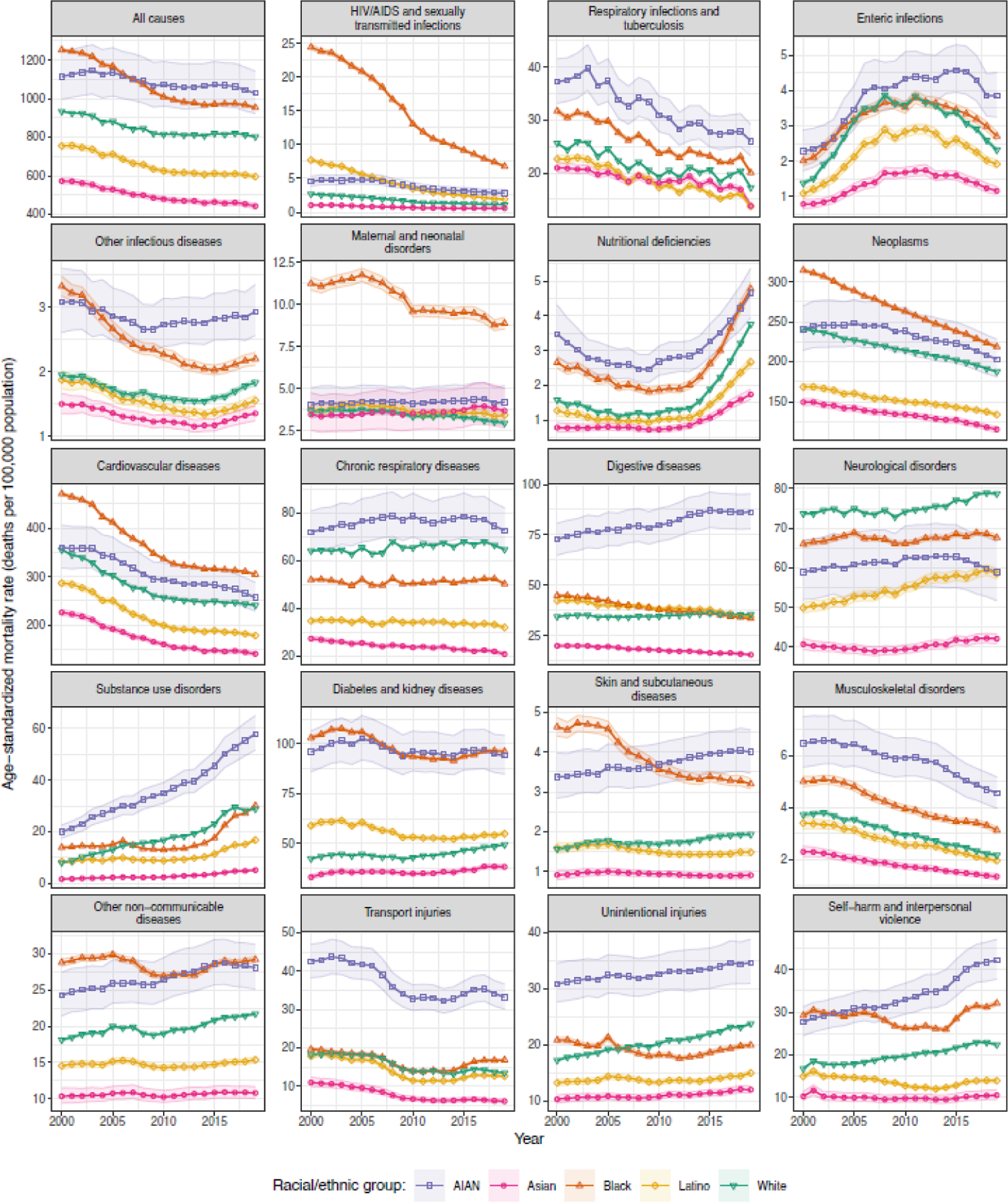
From 2000 to 2019, across 3110 US counties, racial-ethnic disparities in age-standardised mortality were noted for all causes of death considered. Mortality was substantially higher in the AIAN population (all-cause mortality 1028·2 [95% uncertainty interval 922·2-1142·3] per 100 000 population in 2019) and Black population (953·5 [947·5-958·8] per 100 000) than in the White population (802·5 [800·3-804·7] per 100 000), but substantially lower in the Asian population (442·3 [429·3-455·0] per 100 000) and Latino population (595·6 [583·7-606·8] per 100 000), and this pattern was found for most causes of death. However, there were exceptions to this pattern, and the exact order among racial-ethnic groups, magnitude of the disparity in both absolute and relative terms, and change over time in this magnitude varied considerably by cause of death. Similarly, substantial geographical variation in mortality was observed for all causes of death, both overall and within each racial-ethnic group. Racial-ethnic disparities observed at the national level reflect widespread disparities at the county level, although the magnitude of these disparities varied widely among counties. Certain patterns of disparity were nearly universal among counties; for example, in 2019, mortality was higher among the AIAN population than the White population in at least 95% of counties for skin and subcutaneous diseases (455 [97·8%] of 465 counties with unmasked estimates) and HIV/AIDS and sexually transmitted infections (458 [98·5%] counties), and mortality was higher among the Black population than the White population in nearly all counties for skin and subcutaneous diseases (1436 [96·6%] of 1486 counties), diabetes and kidney diseases (1473 [99·1%]), maternal and neonatal disorders (1486 [100·0%] counties), and HIV/AIDS and sexually transmitted infections (1486 [100·0%] counties).
Disparities in mortality among racial-ethnic groups are ubiquitous, occurring across locations in the USA and for a wide range of health conditions. There is an urgent need to address the shared structural factors driving these widespread disparities.
National Institute on Minority Health and Health Disparities; National Heart, Lung, and Blood Institute; National Cancer Institute; National Institute on Aging; National Institute of Arthritis and Musculoskeletal and Skin Diseases; Office of Disease Prevention; and Office of Behavioral and Social Sciences Research, US National Institutes of Health.
在美国,不同种族-族裔群体和地理位置之间的死亡率存在巨大差异,但种族-族裔差异在多大程度上因地理位置而异,或者这些模式如何因死亡原因而异,目前还不太清楚。我们的目的是按种族-族裔、县和死因估算标准化死亡率,并描述美国种族-族裔和基于地点的死亡率之间的交集,比较不同健康状况下的模式。
我们应用小区域估计模型,利用来自美国国家生命统计系统的死亡证明数据和美国国家卫生统计中心的人口数据,估算 2000 年至 2019 年期间 19 种广泛死因的年龄、性别、县和种族-族裔的死亡率。种族和族裔被归类为非拉丁裔和非西班牙裔美国印第安人或阿拉斯加原住民(AIAN)、非拉丁裔和非西班牙裔亚洲或太平洋岛民(亚洲)、非拉丁裔和非西班牙裔黑种人(黑人)、拉丁裔或西班牙裔(拉丁裔)以及非拉丁裔和非西班牙裔白种人(白人)。我们调整了这些死亡率,以纠正死亡证明上种族和族裔报告的错误,并使用直接标准化方法生成年龄标准化结果,以 2010 年美国人口普查人口为标准。
从 2000 年至 2019 年,在 3110 个美国县中,所有考虑的死因的年龄标准化死亡率都存在种族-族裔差异。在 AIAN 人群(2019 年每 10 万人中有 1028.2 [95%置信区间 922.2-1142.3])和黑人人群(953.5 [947.5-958.8])中死亡率明显更高,而在白人人群(802.5 [800.3-804.7])中死亡率明显更低,但在亚洲人群(442.3 [429.3-455.0])和拉丁裔人群(595.6 [583.7-606.8])中死亡率明显更低。对于大多数死因,也存在这种模式。然而,也存在例外情况,种族-族裔群体之间的具体顺序、绝对和相对差异的大小,以及这种差异在时间上的变化,因死因而异。同样,所有死因的死亡率都存在很大的地域差异,无论是整体还是在每个种族-族裔群体中。在全国范围内观察到的种族-族裔差异反映了在县一级普遍存在的差异,尽管这些差异的大小在各县之间差异很大。在某些情况下,差异模式在各县中几乎是普遍存在的;例如,在 2019 年,在至少 95%的县中,皮肤和皮下疾病(465 个县中有 455 个县的未掩盖估计值)和艾滋病毒/艾滋病和性传播感染(465 个县)的死亡率在 AIAN 人群中高于白人人群,而在几乎所有县中,皮肤和皮下疾病(1486 个县中的 1436 个)、糖尿病和肾脏疾病(1473 个县中的 1473 个)、产妇和新生儿疾病(1486 个县中的 1486 个)以及艾滋病毒/艾滋病和性传播感染(1486 个县中的 1486 个)的死亡率在黑人人群中高于白人人群。
不同种族-族裔群体之间的死亡率差异无处不在,发生在美国各地,涉及多种健康状况。迫切需要解决导致这些广泛差异的共同结构性因素。
美国国家少数民族健康和健康差异研究所;国家心脏、肺和血液研究所;国家癌症研究所;国家老龄问题研究所;国家关节炎和肌肉骨骼及皮肤病研究所;疾病预防办公室;以及行为和社会科学研究办公室,美国国立卫生研究院。