Department of Radiation Oncology, Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts, USA.
Department of Radiation Oncology, Memorial Sloan Kettering Cancer Center, New York, New York, USA.
Cancer Rep (Hoboken). 2023 Oct;6(10):e1880. doi: 10.1002/cnr2.1880. Epub 2023 Aug 16.
Testicular cancer (TC) mortality rates have decreased over time, however it is unclear whether these improvements are consistent across all communities.
The aim of this study was to analyze trends in TC incidence, mortality, and place of death (PoD) in the United States between 1999-2020 and identify disparities across race, ethnicity, and geographic location.
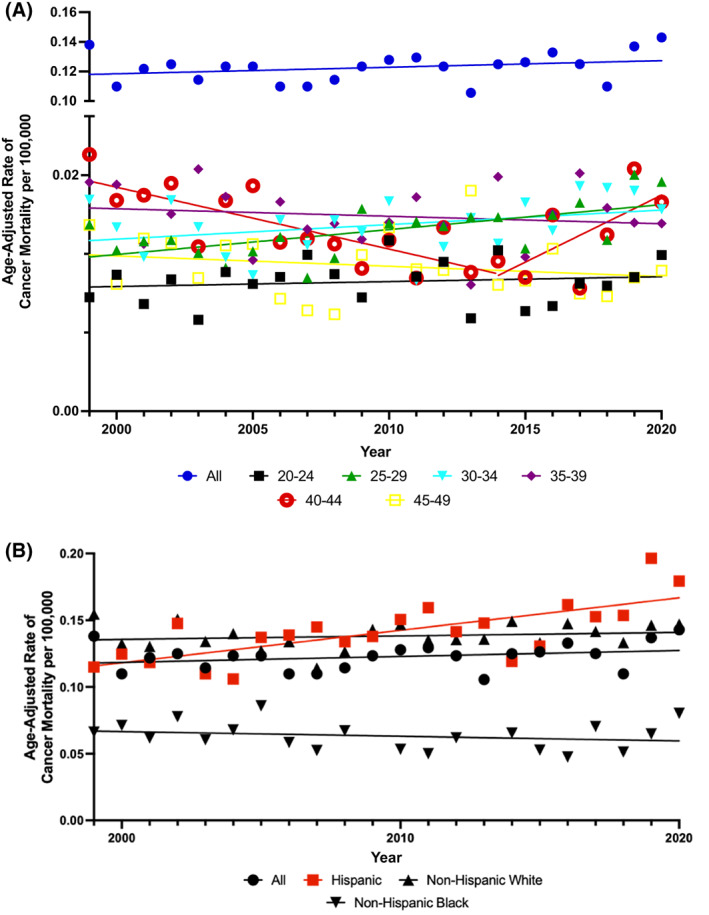
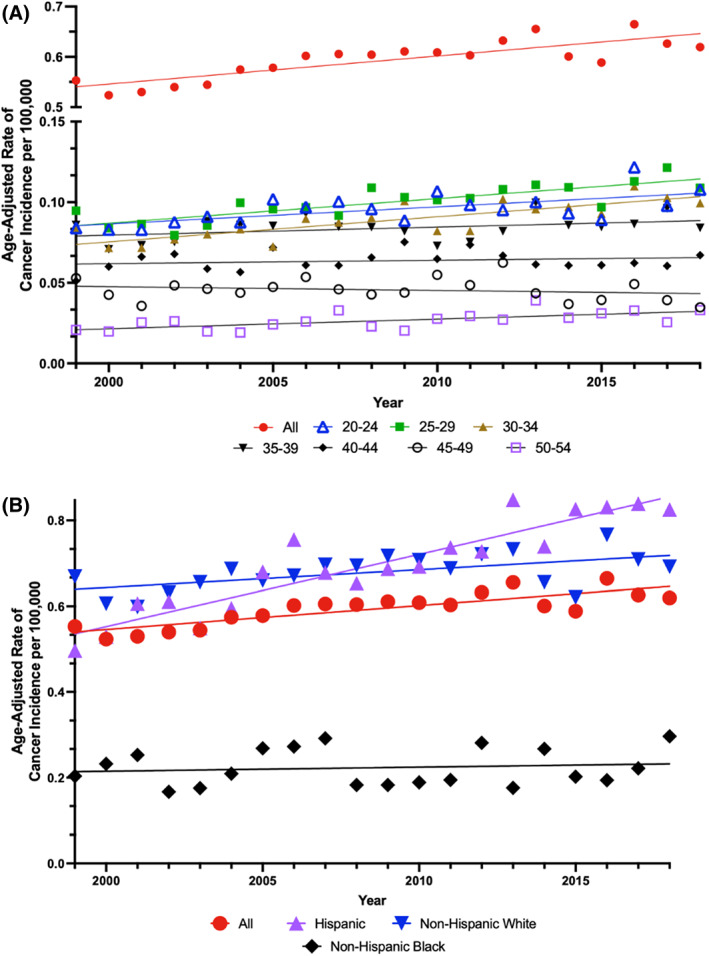
This cross-sectional study used CDC WONDER and NAACCR, to calculate age-adjusted rates of TC incidence and mortality, respectively. PoD data for individuals who died of TC were collected from CDC WONDER. Using Joinpoint analysis, longitudinal mortality trends were evaluated by age, race, ethnicity, US census region, and urbanization category. TC stage (localized vs metastatic) trends were also evaluated. Univariate and multivariate regression analysis identified demographic disparities for PoD. A total of 8,456 patients died of TC from 1999-2020. Average annual percent change (AAPC) of testicular cancer-specific mortality (TCSM) remained largely stable (AAPC, 0.4; 95% CI -0.2 to 0.9; p = 0.215). Men ages 25-29 experienced a significant increase in TCSM (AAPC, 1.3, p = 0.003), consistent with increased metastatic testicular cancer-specific incidence (TCSI) trend for this age group (AAPC, 1.6; p < 0.01). Mortality increased for Hispanic men (AAPC, 1.7, p < 0.001), with increased metastatic TCSI (AAPC, 2.5; p < 0.001). Finally, younger (<45), single, and Hispanic or Black men were more likely to die in medical facilities (all p < 0.001). The retrospective study design is a limitation.
Significant increases in metastatic TC were found for Hispanic men and men aged 25-29 potentially driving increasing testicular cancer specific mortality in these groups. Evidence of racial and ethnic differences in place of death may also highlight treatment disparities.
睾丸癌(TC)的死亡率随着时间的推移而下降,但尚不清楚这些改善是否在所有社区都一致。
本研究旨在分析 1999 年至 2020 年美国 TC 发病率、死亡率和死亡地点(PoD)的趋势,并确定不同种族、族裔和地理位置之间的差异。
这项横断面研究使用 CDC WONDER 和 NAACCR,分别计算 TC 发病率和死亡率的年龄调整率。从 CDC WONDER 收集了死于 TC 的个体的 PoD 数据。使用 Joinpoint 分析,按年龄、种族、族裔、美国人口普查区域和城市化类别评估纵向死亡率趋势。还评估了 TC 分期(局限性与转移性)趋势。单变量和多变量回归分析确定了 PoD 的人口统计学差异。1999 年至 2020 年期间,共有 8456 例患者死于 TC。睾丸癌特异性死亡率(TCSM)的平均年百分比变化(AAPC)基本保持稳定(AAPC,0.4;95%CI-0.2 至 0.9;p=0.215)。25-29 岁男性的 TCSM 显著增加(AAPC,1.3,p=0.003),与该年龄组转移性睾丸癌特异性发病率(TCSI)趋势一致(AAPC,1.6;p<0.01)。西班牙裔男性的死亡率增加(AAPC,1.7,p<0.001),转移性 TCSI 增加(AAPC,2.5;p<0.001)。最后,年龄较小(<45 岁)、单身和西班牙裔或黑人男性更有可能在医疗机构死亡(均 p<0.001)。回顾性研究设计是一个限制。
西班牙裔男性和 25-29 岁男性的转移性 TC 显著增加,可能导致这些人群的睾丸癌特异性死亡率增加。死亡地点的种族和族裔差异的证据也可能突出了治疗差异。