Medical Faculty, University of Leipzig, Leipzig, Germany.
Department of Neurology, Zaozhuang Municipal Hospital, Shandong, China.
Front Immunol. 2023 Aug 4;14:1191130. doi: 10.3389/fimmu.2023.1191130. eCollection 2023.
Significant evidence suggests that asthma might originate from low-grade systemic inflammation. Previous studies have established a positive association between the systemic immune-inflammation index (SII) and the systemic inflammation response index (SIRI) levels and the risk of stroke. However, it remains unclear whether SII, SIRI and the prevalence of stroke are related in individuals with asthma.
The present cross-sectional study used data from the National Health and Nutrition Examination Survey (NHANES) conducted between 1999 and 2018. SII was calculated using the following formula: (platelet count neutrophil count)lymphocyte count. SIRI was calculated using the following formula: (neutrophil count × monocyte count)/lymphocyte count. The Spearman rank correlation coefficient was used to determine any correlation between SII, SIRI, and the baseline characteristics. Survey-weighted logistic regression was employed to calculate odds ratios (ORs) and 95% confidence intervals (CIs) to determine the association between SII, SIRI, and stroke prevalence. The predictive value of SII and SIRI for stroke prevalence was assessed through receiver operating characteristic (ROC) curve analysis, with the area under the ROC curve (AUC) being indicative of its predictive value. Additionally, clinical models including SIRI, coronary heart disease, hypertension, age, and poverty income ratio were constructed to evaluate their clinical applicability.
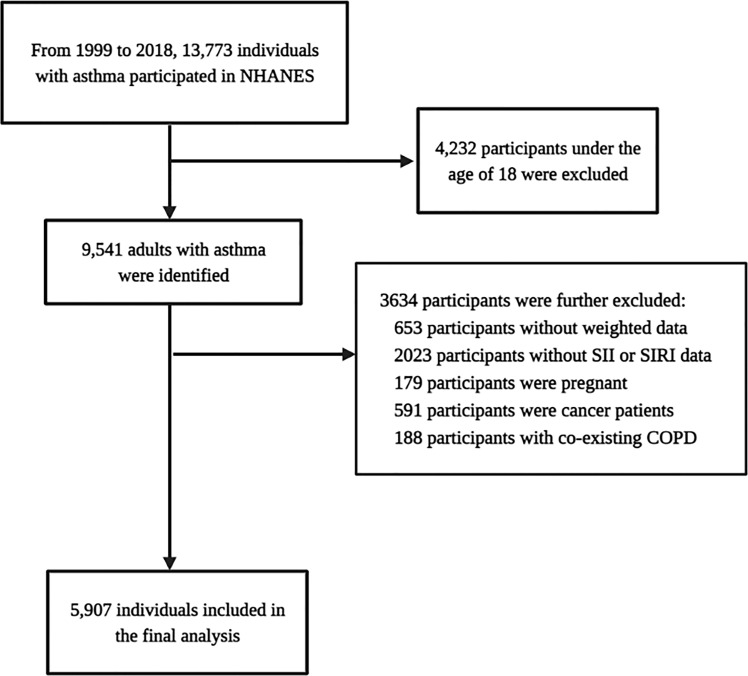
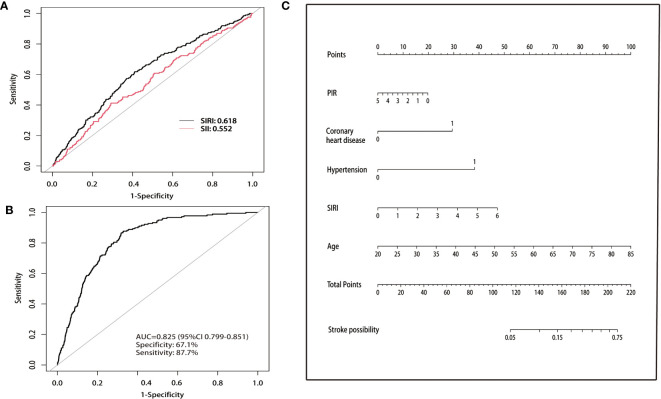
Between 1999 and 2018, 5,907 NHANES participants with asthma were identified, of which 199 participants experienced a stroke, while the remaining 5,708 participants had not. Spearman rank correlation analysis indicated that neither SII nor SIRI levels exhibited any significant correlation with the baseline characteristics of the participants (r<0.1). ROC curves were used to determine the optimal cut-off values for SII and SIRI levels to classify participants into low- and high-level groups. Higher SII and SIRI levels were associated with a higher prevalence of stroke, with ORs of 1.80 (95% CI, 1.18-2.76) and 2.23 (95% CI, 1.39-3.57), respectively. The predictive value of SIRI (AUC=0.618) for stroke prevalence was superior to that of SII (AUC=0.552). Furthermore, the clinical model demonstrated good predictive value (AUC=0.825), with a sensitivity of 67.1% and specificity of 87.7%.
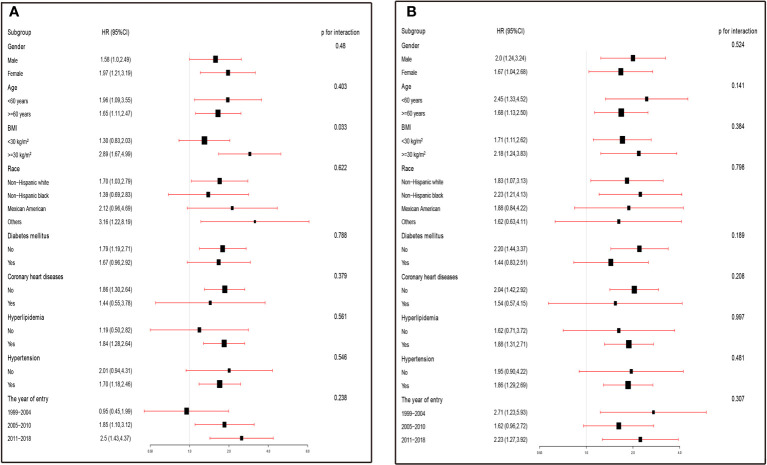
In asthmatics, higher levels of SII and SIRI significantly increased the prevalence of stroke, with its association being more pronounced in individuals with coexisting obesity and hyperlipidaemia. SII and SIRI are relatively stable novel inflammatory markers in the asthmatic population, with SIRI having a better predictive value for stroke prevalence than SII.
大量证据表明,哮喘可能源于低度全身炎症。先前的研究已经确定了全身免疫炎症指数(SII)和全身炎症反应指数(SIRI)水平与中风风险之间的正相关关系。然而,目前尚不清楚哮喘患者的 SII、SIRI 和中风患病率之间是否存在关联。
本横断面研究使用了 1999 年至 2018 年期间进行的国家健康和营养检查调查(NHANES)的数据。SII 是通过以下公式计算得出的:(血小板计数×中性粒细胞计数)淋巴细胞计数。SIRI 是通过以下公式计算得出的:(中性粒细胞计数×单核细胞计数)淋巴细胞计数。Spearman 秩相关系数用于确定 SII、SIRI 和基线特征之间的任何相关性。采用调查加权逻辑回归计算 SII、SIRI 与中风患病率之间的比值比(OR)和 95%置信区间(CI),以确定 SII、SIRI 与中风患病率之间的关联。通过接收者操作特征(ROC)曲线分析评估 SII 和 SIRI 对中风患病率的预测价值,ROC 曲线下面积(AUC)表示其预测价值。此外,构建了包含 SIRI、冠心病、高血压、年龄和贫困收入比的临床模型,以评估其临床适用性。
在 1999 年至 2018 年期间,确定了 5907 名患有哮喘的 NHANES 参与者,其中 199 名参与者发生了中风,而其余 5708 名参与者未发生中风。Spearman 秩相关分析表明,SII 和 SIRI 水平均与参与者的基线特征无显著相关性(r<0.1)。ROC 曲线用于确定 SII 和 SIRI 水平的最佳截断值,以将参与者分为低水平组和高水平组。较高的 SII 和 SIRI 水平与较高的中风患病率相关,OR 值分别为 1.80(95%CI,1.18-2.76)和 2.23(95%CI,1.39-3.57)。SIRI(AUC=0.618)对中风患病率的预测价值优于 SII(AUC=0.552)。此外,临床模型表现出良好的预测价值(AUC=0.825),灵敏度为 67.1%,特异性为 87.7%。
在哮喘患者中,较高的 SII 和 SIRI 水平显著增加了中风的患病率,在同时存在肥胖和高脂血症的患者中,这种关联更为明显。SII 和 SIRI 是哮喘人群中相对稳定的新型炎症标志物,SIRI 对中风患病率的预测价值优于 SII。