Department of Anesthesiology, The Third Affiliated Hospital of Shenzhen University, Shenzhen, China.
The First School of Clinical Medicine, Guangdong Medical University, Zhanjiang, China.
Medicine (Baltimore). 2023 Oct 13;102(41):e35467. doi: 10.1097/MD.0000000000035467.
Anesthetic management during resection of pheochromocytoma is a huge challenge, especially when accompanied by dilated cardiomyopathy (DCM). However, there is a lack of research evidence in this area.
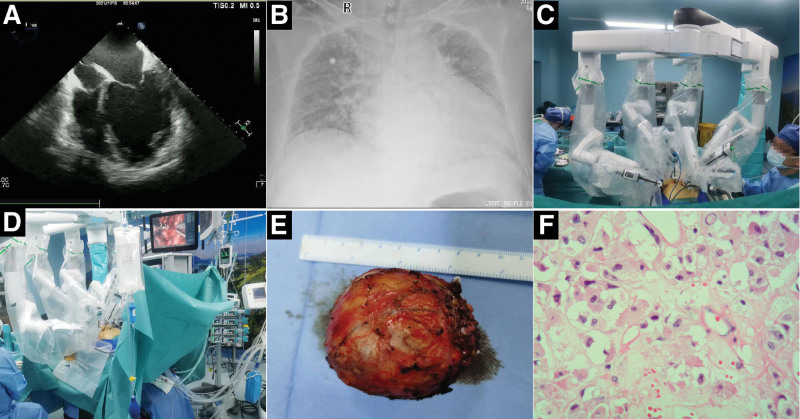
A 36-year-old man was admitted with a left retroperitoneal space-occupying lesion, present for 2 years. The patient also had DCM for 2 years. Blood analysis on admission showed elevated levels of norepinephrine and the N-terminus of the brain natriuretic peptide precursor. Abdominal computed tomography revealed a circular shadow in the left adrenal area. Echocardiography showed a cardiac ejection fraction of 31% to 37%, markedly enlarged left atrium and left ventricle, extensive cardiac hypokinesia, and reduced left ventricular diastolic and systolic functions.
The preoperative diagnosis was left paraganglioma/pheochromocytoma with DCM.
Multidisciplinary consultation, blood pressure measurements, and volume expansion measurements were performed preoperatively. Invasive arterial blood pressure, central venous pressure, depth of anesthesia, cardiac function, left heart volume, and body temperature were monitored intraoperatively.
The adrenal pheochromocytoma was successfully removed, and the patient recovered well.
The anesthetic management for adrenal pheochromocytoma resection in adult patients with DCM is extremely high-risk but is evidently not impossible. Adequate preoperative evaluation and preparation, optimization of the anesthesia induction plan, close intraoperative monitoring of cardiac function and hemodynamic changes, and robot-assisted laparoscopic technology are the key success factors. The challenges to anesthetic management may be partly prevented with invasive monitoring techniques and minimally invasive surgery. This case confirms the importance of individual management and multidisciplinary cooperation for a successful outcome.
在切除嗜铬细胞瘤时,麻醉管理极具挑战性,尤其是在伴有扩张型心肌病(DCM)时。然而,这方面的研究证据不足。
一名 36 岁男性因左腹膜后占位性病变入院,该病变已存在 2 年。患者同时患有 DCM 2 年。入院时的血液分析显示去甲肾上腺素和脑利钠肽前体 N 端水平升高。腹部 CT 显示左肾上腺区有圆形阴影。超声心动图显示心脏射血分数为 31%至 37%,左心房和左心室明显增大,广泛的心脏运动功能减退,左心室舒张和收缩功能降低。
术前诊断为左副神经节瘤/嗜铬细胞瘤伴 DCM。
术前进行多学科会诊、血压测量和容量扩张测量。术中进行有创动脉血压、中心静脉压、麻醉深度、心功能、左心容量和体温监测。
成功切除肾上腺嗜铬细胞瘤,患者恢复良好。
成人 DCM 患者行肾上腺嗜铬细胞瘤切除术的麻醉管理风险极高,但并非不可能。充分的术前评估和准备、优化麻醉诱导方案、密切监测术中心功能和血流动力学变化以及机器人辅助腹腔镜技术是关键的成功因素。有创监测技术和微创手术可能部分预防麻醉管理的挑战。该病例证实了个体化管理和多学科合作对于获得良好结果的重要性。