Department of General Midwifery, School of Midwifery, College of Medicine & Health sciences, University of Gondar, Gondar, Ethiopia.
Department of Women's and Family Health, School of midwifery, College of Medicine & Health sciences, University of Gondar, Gondar, Ethiopia.
BMC Pregnancy Childbirth. 2023 Oct 17;23(1):732. doi: 10.1186/s12884-023-06018-1.
Prematurity is the leading cause of neonatal morbidity and mortality, specifically in low-resource settings. The majority of prematurity can be prevented if early interventions are implemented for high-risk pregnancies. Developing a prognosis risk score for preterm birth based on easily available predictors could support health professionals as a simple clinical tool in their decision-making. Therefore, the study aims to develop and validate a prognosis risk score model for preterm birth among pregnant women who had antenatal care visit at Debre Markos Comprehensive and Specialized Hospital, Ethiopia.
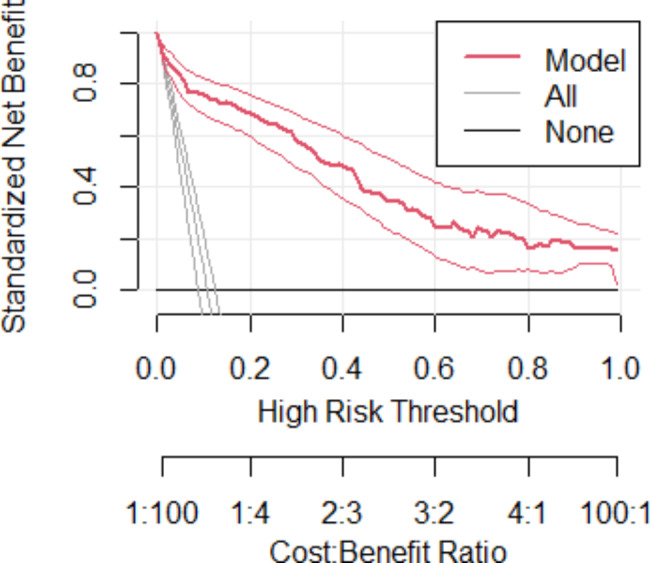
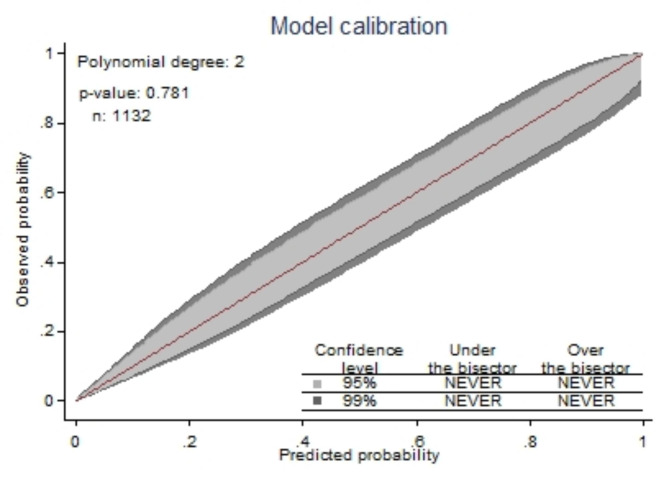
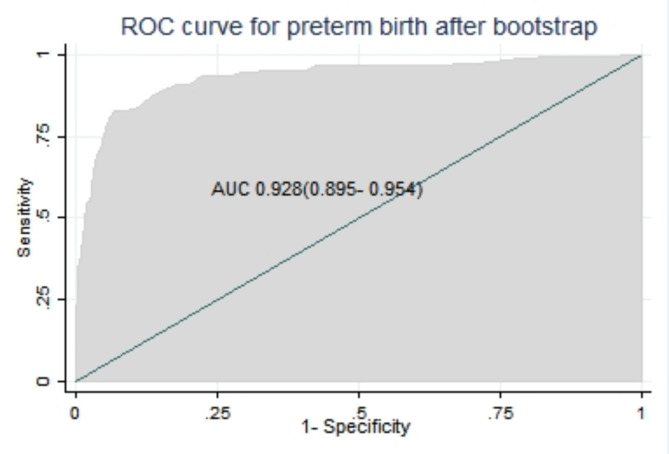
A retrospective follow-up study was conducted among a total of 1,132 pregnant women. Client charts were selected using a simple random sampling technique. Data were extracted using structured checklist prepared in the Kobo Toolbox application and exported to STATA version 14 and R version 4.2.2 for data management and analysis. Stepwise backward multivariable analysis was done. A simplified risk prediction model was developed based on a binary logistic model, and the model's performance was assessed by discrimination power and calibration. The internal validity of the model was evaluated by bootstrapping. Decision Curve Analysis was used to determine the clinical impact of the model.
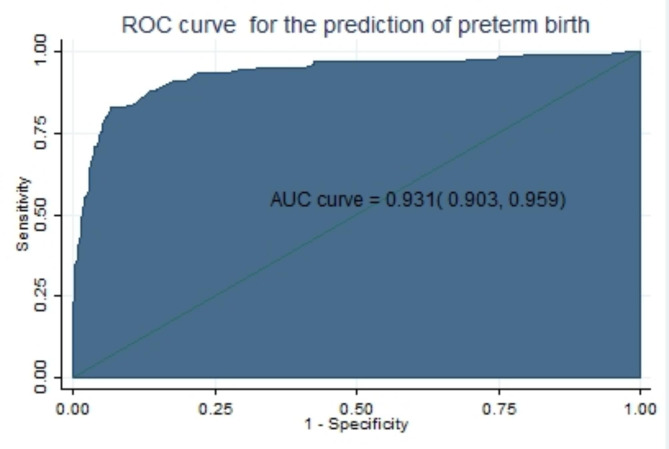
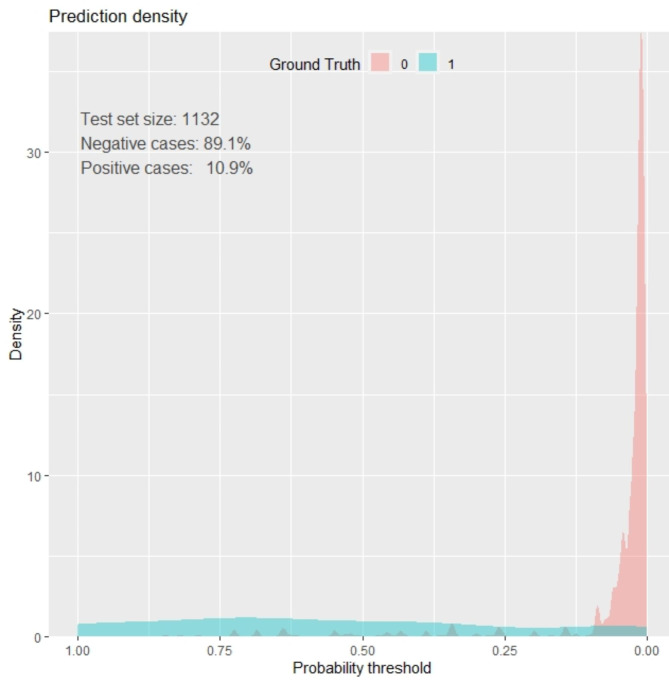
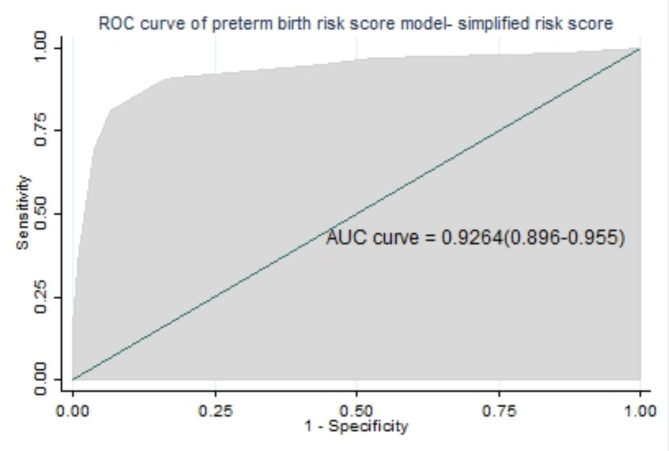
The incidence of preterm birth was 10.9%. The developed risk score model comprised of six predictors that remained in the reduced multivariable logistic regression, including age < 20, late initiation of antenatal care, unplanned pregnancy, recent pregnancy complications, hemoglobin < 11 mg/dl, and multiparty, for a total score of 17. The discriminatory power of the model was 0.931, and the calibration test was p > 0.05. The optimal cut-off for classifying risks as low or high was 4. At this cut point, the sensitivity, specificity and accuracy is 91.0%, 82.1%, and 83.1%, respectively. It was internally validated and has an optimism of 0.003. The model was found to have clinical benefit.
The developed risk-score has excellent discrimination performance and clinical benefit. It can be used in the clinical settings by healthcare providers for early detection, timely decision making, and improving care quality.
早产是导致新生儿发病率和死亡率的主要原因,尤其是在资源匮乏的环境中。如果对高危妊娠实施早期干预,大多数早产是可以预防的。基于易于获得的预测因素,为早产制定预后风险评分,可以为卫生专业人员提供一个简单的临床决策工具。因此,本研究旨在为在埃塞俄比亚德布雷马科斯综合和专科医院接受产前护理的孕妇开发和验证一种早产预后风险评分模型。
这是一项回顾性随访研究,共纳入了 1132 名孕妇。使用简单随机抽样技术从客户病历中选择样本。使用 Kobo Toolbox 应用程序中准备的结构化清单提取数据,并将数据导出到 STATA 版本 14 和 R 版本 4.2.2 进行数据管理和分析。采用逐步向后多变量分析。基于二项逻辑回归模型建立简化风险预测模型,并通过区分能力和校准评估模型性能。通过自举法评估模型的内部有效性。决策曲线分析用于确定模型的临床影响。
早产发生率为 10.9%。所开发的风险评分模型包含六个预测因子,这些因子在多元逻辑回归中仍然存在,包括年龄<20 岁、晚期开始产前护理、非计划妊娠、近期妊娠并发症、血红蛋白<11mg/dl 和多胎妊娠,总分为 17 分。模型的区分能力为 0.931,校准检验 p>0.05。将风险分类为低风险或高风险的最佳截断值为 4。在该截断点,敏感性、特异性和准确性分别为 91.0%、82.1%和 83.1%。该模型经过内部验证,且存在 0.003 的乐观偏差。该模型具有临床获益。
所开发的风险评分具有出色的区分性能和临床获益。它可以由医疗保健提供者在临床环境中使用,用于早期发现、及时决策和提高护理质量。