Nguyen Kim-Anh-Nhi, Tandon Pranai, Ghanavati Sahar, Cheetirala Satya Narayana, Timsina Prem, Freeman Robert, Reich David, Levin Matthew A, Mazumdar Madhu, Fayad Zahi A, Kia Arash
Institute for Healthcare Delivery Science, Icahn School of Medicine at Mount Sinai, New York, NY, United States.
Department of Medicine Division of Pulmonary, Critical Care, and Sleep Medicine, Icahn School of Medicine at Mount Sinai, New York, NY, United States.
JMIR Form Res. 2023 Oct 26;7:e46905. doi: 10.2196/46905.
Early prediction of the need for invasive mechanical ventilation (IMV) in patients hospitalized with COVID-19 symptoms can help in the allocation of resources appropriately and improve patient outcomes by appropriately monitoring and treating patients at the greatest risk of respiratory failure. To help with the complexity of deciding whether a patient needs IMV, machine learning algorithms may help bring more prognostic value in a timely and systematic manner. Chest radiographs (CXRs) and electronic medical records (EMRs), typically obtained early in patients admitted with COVID-19, are the keys to deciding whether they need IMV.
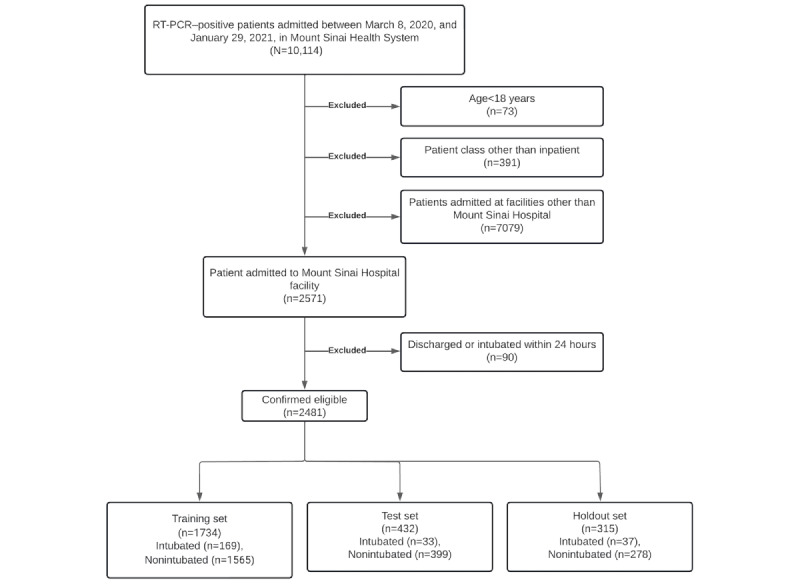
We aimed to evaluate the use of a machine learning model to predict the need for intubation within 24 hours by using a combination of CXR and EMR data in an end-to-end automated pipeline. We included historical data from 2481 hospitalizations at The Mount Sinai Hospital in New York City.
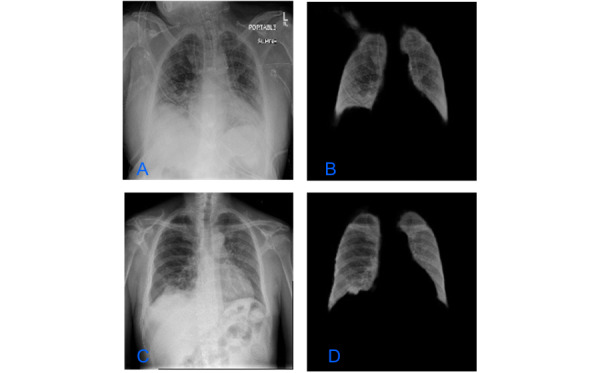
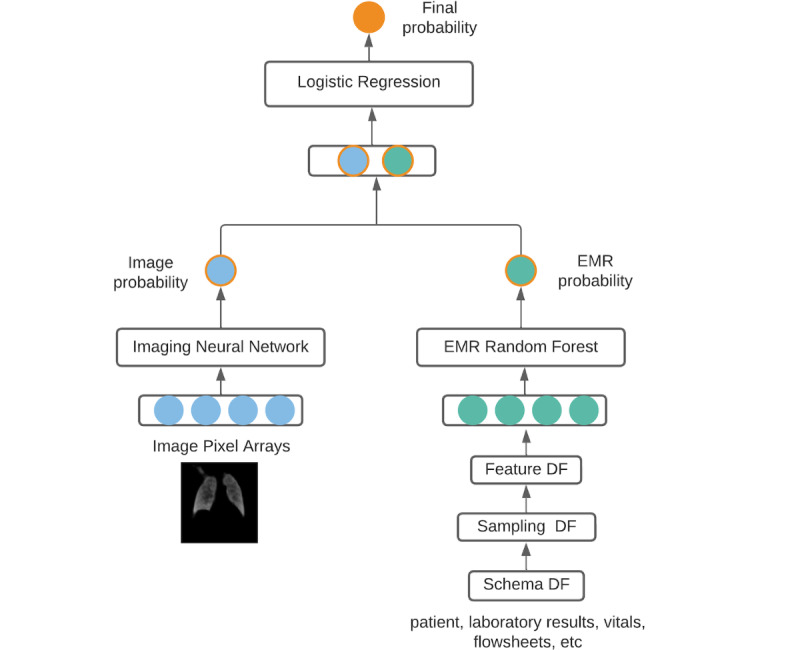
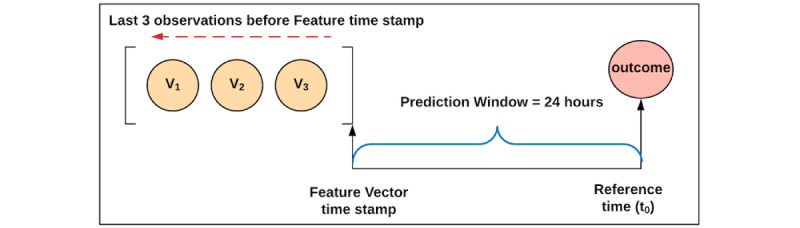
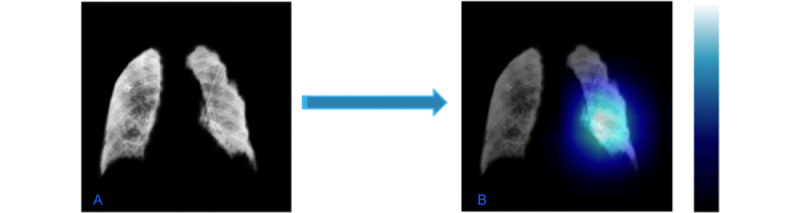
CXRs were first resized, rescaled, and normalized. Then lungs were segmented from the CXRs by using a U-Net algorithm. After splitting them into a training and a test set, the training set images were augmented. The augmented images were used to train an image classifier to predict the probability of intubation with a prediction window of 24 hours by retraining a pretrained DenseNet model by using transfer learning, 10-fold cross-validation, and grid search. Then, in the final fusion model, we trained a random forest algorithm via 10-fold cross-validation by combining the probability score from the image classifier with 41 longitudinal variables in the EMR. Variables in the EMR included clinical and laboratory data routinely collected in the inpatient setting. The final fusion model gave a prediction likelihood for the need of intubation within 24 hours as well.
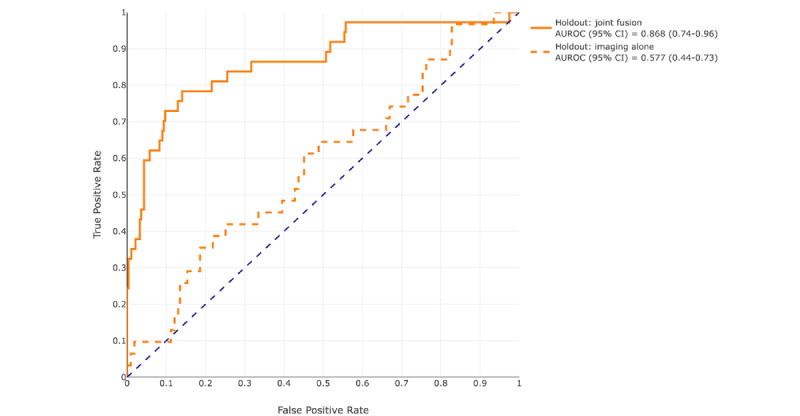
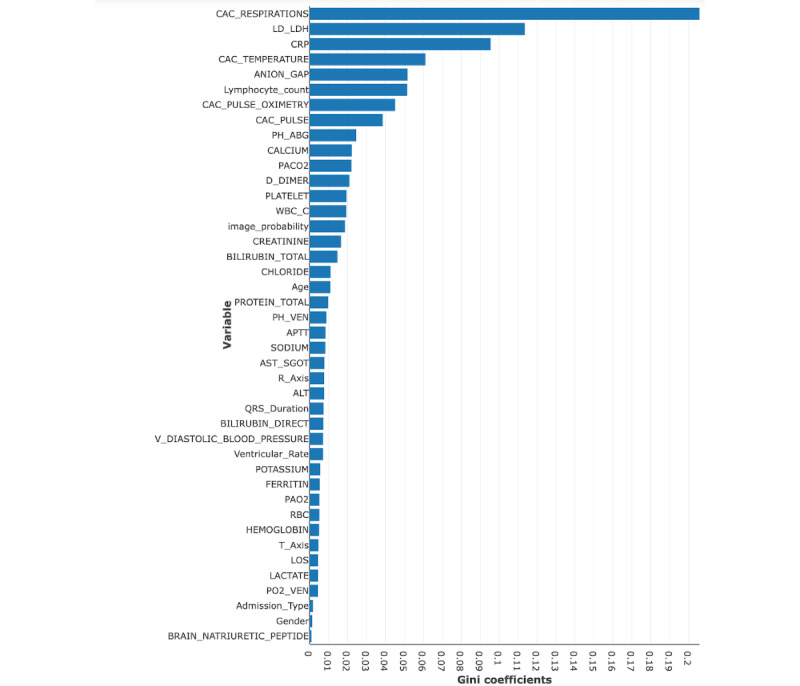
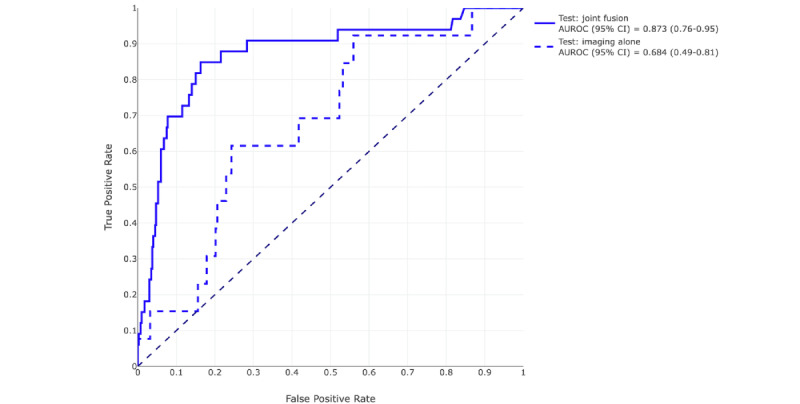
At a prediction probability threshold of 0.5, the fusion model provided 78.9% (95% CI 59%-96%) sensitivity, 83% (95% CI 76%-89%) specificity, 0.509 (95% CI 0.34-0.67) F-score, 0.874 (95% CI 0.80-0.94) area under the receiver operating characteristic curve (AUROC), and 0.497 (95% CI 0.32-0.65) area under the precision recall curve (AUPRC) on the holdout set. Compared to the image classifier alone, which had an AUROC of 0.577 (95% CI 0.44-0.73) and an AUPRC of 0.206 (95% CI 0.08-0.38), the fusion model showed significant improvement (P<.001). The most important predictor variables were respiratory rate, C-reactive protein, oxygen saturation, and lactate dehydrogenase. The imaging probability score ranked 15th in overall feature importance.
We show that, when linked with EMR data, an automated deep learning image classifier improved performance in identifying hospitalized patients with severe COVID-19 at risk for intubation. With additional prospective and external validation, such a model may assist risk assessment and optimize clinical decision-making in choosing the best care plan during the critical stages of COVID-19.
对出现新型冠状病毒肺炎(COVID-19)症状住院患者是否需要有创机械通气(IMV)进行早期预测,有助于合理分配资源,并通过对呼吸衰竭风险最高的患者进行适当监测和治疗来改善患者预后。为应对判断患者是否需要IMV的复杂性,机器学习算法可能有助于及时、系统地提供更多预后价值。胸部X光片(CXR)和电子病历(EMR)通常在COVID-19入院患者早期获取,是决定他们是否需要IMV的关键。
我们旨在评估使用机器学习模型,通过在端到端自动化流程中结合CXR和EMR数据,预测24小时内是否需要插管。我们纳入了纽约市西奈山医院2481例住院病例的历史数据。
首先对CXR进行调整大小、重新缩放和归一化。然后使用U-Net算法从CXR中分割出肺部。将其分为训练集和测试集后,对训练集图像进行增强。通过迁移学习、10折交叉验证和网格搜索,对预训练的DenseNet模型进行重新训练,使用增强后的图像训练图像分类器,以预测24小时预测窗口内插管的概率。然后,在最终融合模型中,通过将图像分类器的概率得分与EMR中的41个纵向变量相结合,使用10折交叉验证训练随机森林算法。EMR中的变量包括住院环境中常规收集的临床和实验室数据。最终融合模型也给出了24小时内需要插管的预测可能性。
在预测概率阈值为0.5时,融合模型在保留集上的灵敏度为78.9%(95%CI 59%-96%),特异性为83%(95%CI 76%-89%),F值为0.509(95%CI 0.34-0.67),受试者操作特征曲线下面积(AUROC)为0.874(95%CI 0.80-0.94),精确召回率曲线下面积(AUPRC)为0.497(95%CI 0.32-0.65)。与单独的图像分类器相比,其AUROC为0.577(95%CI 0.44-0.73),AUPRC为0.206(95%CI 0.08-0.38),融合模型有显著改善(P<.001)。最重要的预测变量是呼吸频率、C反应蛋白、血氧饱和度和乳酸脱氢酶。成像概率得分在总体特征重要性中排名第15。
我们表明,当与EMR数据相关联时,自动化深度学习图像分类器在识别有插管风险的重症COVID-19住院患者方面提高了性能。经过额外的前瞻性和外部验证,这样的模型可能有助于风险评估,并在COVID-19关键阶段优化临床决策,以选择最佳护理方案。