Huang Yan, Zhang Han, Hu Xueping, Qin Shanshan, Hu Fan, Li Yuchen, Cai Haidong, Shi Kuangyu, Yu Fei
Medical College, Anhui University of Science and Technology, Huainan, China.
Department of Nuclear Medicine, Shanghai Tenth People's Hospital, Tongji University School of Medicine, Shanghai, China.
EJNMMI Phys. 2024 Jan 8;11(1):5. doi: 10.1186/s40658-023-00606-y.
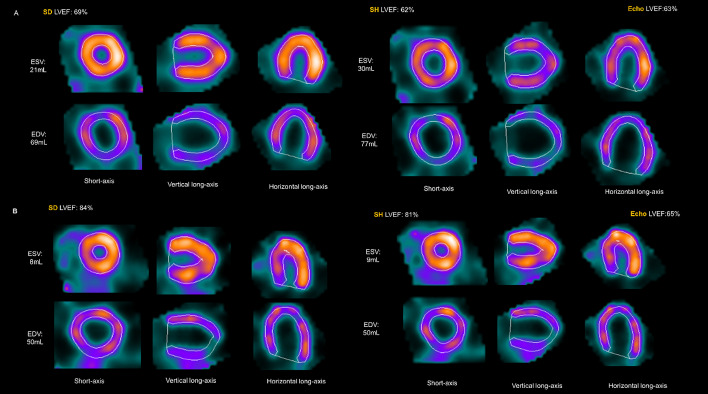
Due to spatial resolution limitations, conventional NaI-SPECT typically overestimates the left ventricular (LV) ejection fraction (EF) in patients with small LV volumes. The purpose of this study was to explore the clinical application value of the small heart (SH) reconstruction protocol embedded in the postprocessing procedure of D-SPECT.
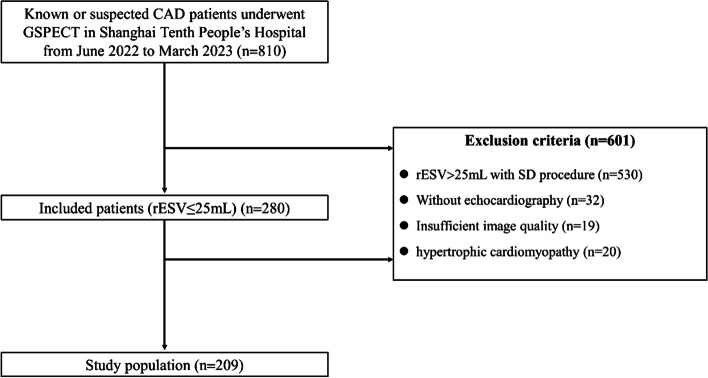
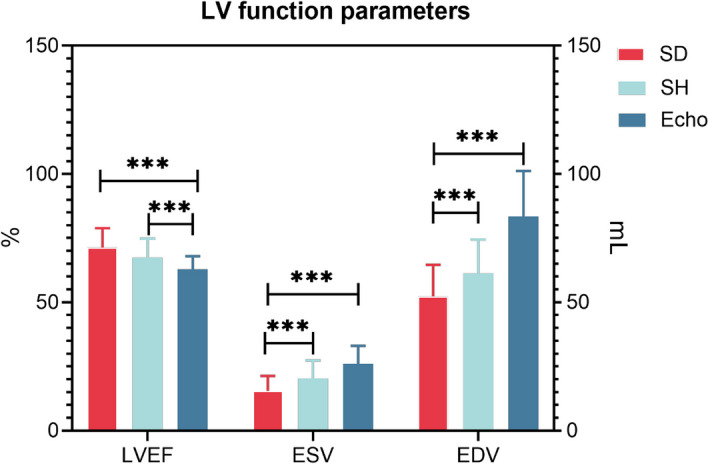
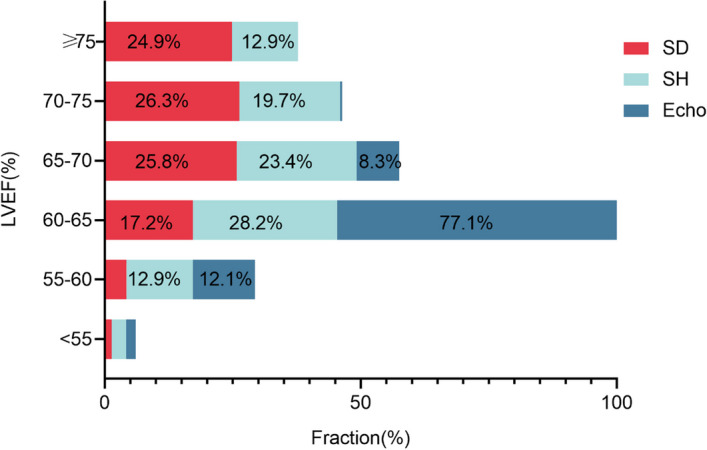
We retrospectively analyzed patients who undergo both D-SPECT and echocardiography (Echo) within one week. Patients with small LV volume were defined as those with a rest end-systolic volume (rESV) ≤ 25 mL and underwent reconstruction using the standard (SD) reconstruction protocol. The SH protocol was deemed successful in correcting the LVEF value if it decreased by 5% or more compared to the SD protocol. The ROC curve was used to calculate the optimal cutoff value of the SH protocol. LVEF, ESV and EDV were computed with SD and SH, respectively. Echo was performed as a reference, and Echo-LVEF, ESV, and EDV were calculated using the Teichholz formula. One-way ANOVA was used to compare these parameters among the three groups.
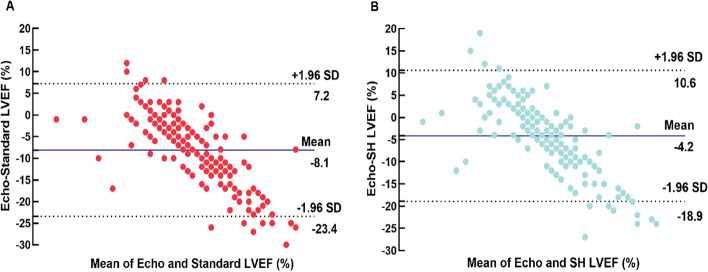
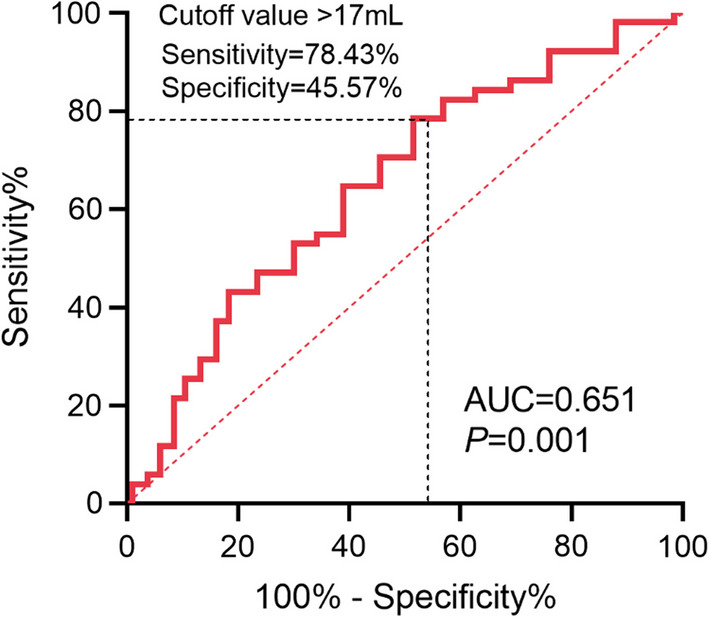
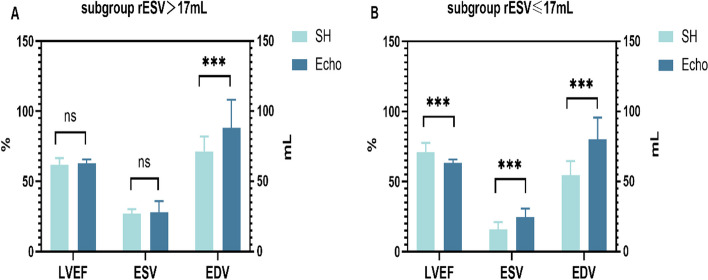
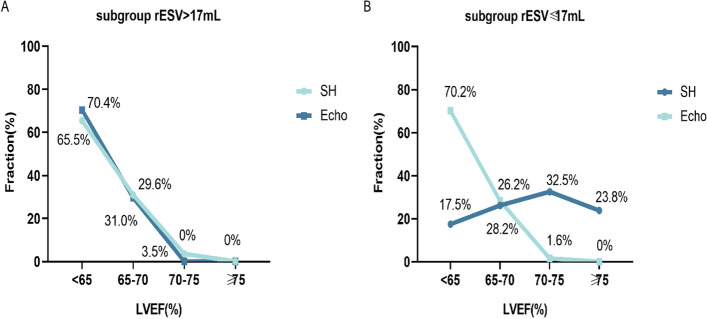
The final study included 209 patients (73.21% female, age 67.34 ± 7.85 years). Compared with the SD protocol, the SH protocol significantly decreased LVEF (67.43 ± 7.38% vs. 71.30 ± 7.61%, p < 0.001). The optimal cutoff value for using the SH protocol was rESV > 17 mL (AUC = 0.651, sensitivity = 78.43%, specificity = 45.57%, p = 0.001). In the subgroup of rESV > 17 mL, there was no significant difference in LVEF (61.84 ± 4.67% vs. 62.83 ± 2.85%, p = 0.481) between the SH protocol and Echo, and no significant difference was observed in rESV (26.92 ± 3.25 mL vs. 27.94 ± 7.96 mL, p = 0.60) between the SH protocol and Echo.
This pilot study demonstrated that the SH reconstruction protocol was able to effectively correct the overestimation of LVEF in patients with small LV volumes. Particularly, in the rESV > 17 mL subgroup, the time and computing power waste could be reduced while still ensuring the accuracy of the LVEF value and image quality.
由于空间分辨率的限制,传统的碘化钠单光子发射计算机断层扫描(NaI-SPECT)通常会高估左心室(LV)容积较小患者的左心室射血分数(EF)。本研究的目的是探讨D-SPECT后处理程序中嵌入的小心脏(SH)重建方案的临床应用价值。
我们回顾性分析了在一周内同时接受D-SPECT和超声心动图(Echo)检查的患者。左心室容积较小的患者定义为静息收缩末期容积(rESV)≤25 mL,并使用标准(SD)重建方案进行重建。如果与SD方案相比,SH方案使左心室射血分数值降低5%或更多,则认为SH方案成功校正了该值。使用ROC曲线计算SH方案的最佳截断值。分别用SD和SH计算左心室射血分数、收缩末期容积和舒张末期容积。以Echo作为参考,使用Teichholz公式计算Echo-左心室射血分数、收缩末期容积和舒张末期容积。采用单因素方差分析比较三组之间的这些参数。
最终纳入研究的患者有209例(女性占73.21%,年龄67.34±7.85岁)。与SD方案相比,SH方案显著降低了左心室射血分数(67.43±7.38% vs. 71.30±7.61%,p<0.001)。使用SH方案的最佳截断值为rESV>17 mL(曲线下面积[AUC]=0.651,灵敏度=78.43%,特异性=45.57%,p=0.001)。在rESV>17 mL的亚组中,SH方案与Echo之间的左心室射血分数无显著差异(61.84±4.67% vs. 62.83±2.85%,p=0.481),SH方案与Echo之间的rESV也无显著差异(26.92±3.25 mL vs. 27.94±7.96 mL,p=0.60)。
这项初步研究表明,SH重建方案能够有效校正左心室容积较小患者左心室射血分数的高估。特别是,在rESV>17 mL的亚组中,在确保左心室射血分数值准确性和图像质量的同时,可以减少时间和计算能力的浪费。