Department of Neurology, Institute of Clinical Medicine, University of Eastern Finland, Kuopio, Finland.
Division of Clinical Geriatrics, Center for Alzheimer Research, Department of Neurobiology, Care Sciences and Society, Karolinska Institutet, Stockholm, Sweden.
Eur J Neurol. 2024 May;31(5):e16238. doi: 10.1111/ene.16238. Epub 2024 Feb 7.
The complex aetiology of Alzheimer's disease suggests prevention potential. Risk scores have potential as risk stratification tools and surrogate outcomes in multimodal interventions targeting specific at-risk populations. The Australian National University Alzheimer's Disease Risk Index (ANU-ADRI) was tested in relation to cognition and its suitability as a surrogate outcome in a multidomain lifestyle randomized controlled trial, in older adults at risk of dementia.
In this post hoc analysis of the Finnish Intervention Study to Prevent Cognitive Impairment and Disability (FINGER), ANU-ADRI was calculated at baseline, 12, and 24 months (n = 1174). The association between ANU-ADRI and cognition (at baseline and over time), the intervention effect on changes in ANU-ADRI, and the potential impact of baseline ANU-ADRI on the intervention effect on changes in cognition were assessed using linear mixed models with maximum likelihood estimation.
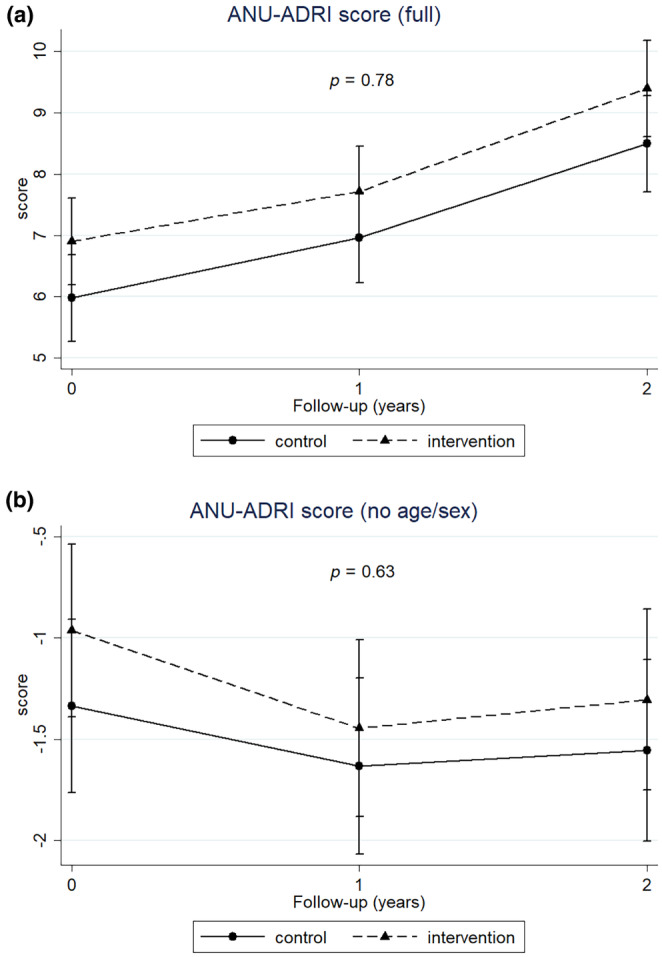
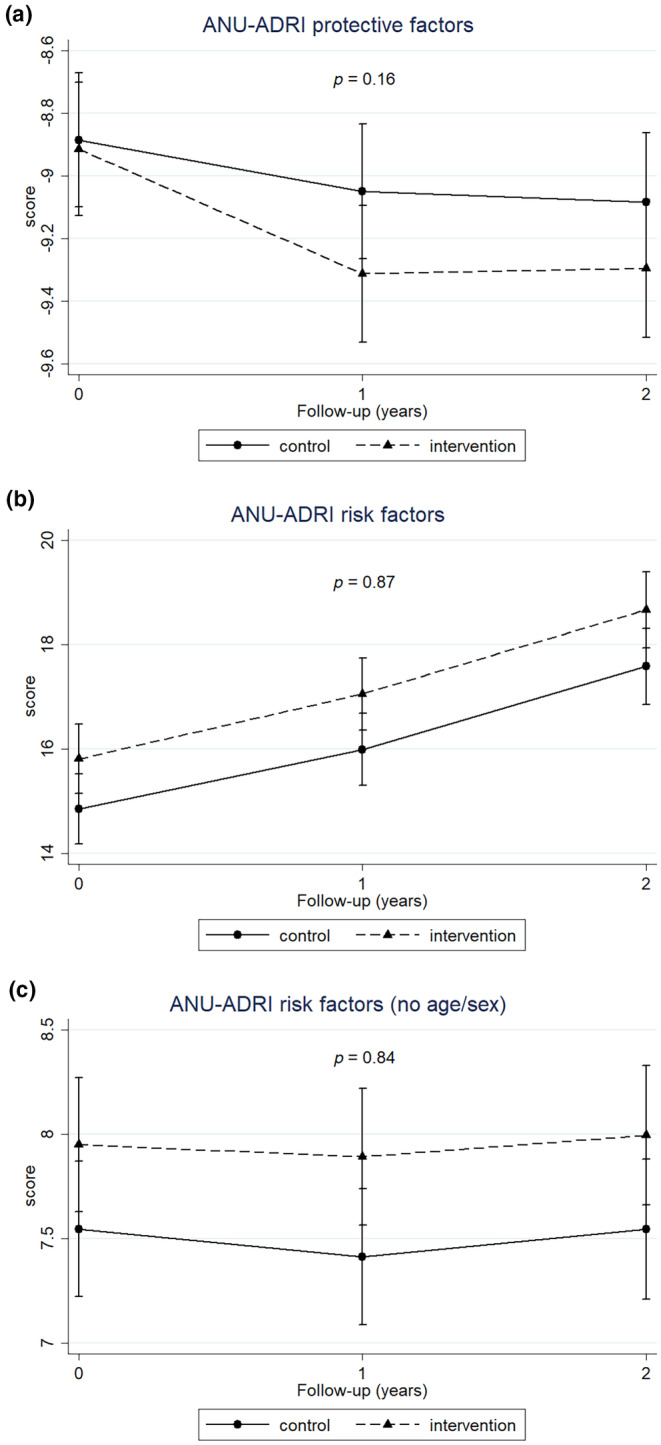
A higher ANU-ADRI was significantly related to worse cognition, at baseline (e.g., estimate for global cognition [95% confidence interval] was -0.028 [-0.032 to -0.025]) and over the 2-year study (e.g., estimate for 2-year changes in ANU-ADRI and per-year changes in global cognition [95% confidence interval] was -0.068 [-0.026 to -0.108]). No significant beneficial intervention effect was reported for ANU-ADRI, and baseline ANU-ADRI did not significantly affect the response to the intervention on changes in cognition.
The ANU-ADRI was effective for the risk prediction of cognitive decline. Risk scores may be crucial for the success of novel dementia prevention strategies, but their algorithm, the target population, and the intervention design should be carefully considered when choosing the appropriate tool for each context.
阿尔茨海默病的复杂病因表明其具有潜在的可预防性。风险评分具有作为风险分层工具和针对特定高危人群的多模态干预替代终点的潜力。澳大利亚国立大学阿尔茨海默病风险指数(ANU-ADRI)已在认知方面进行了测试,并在针对痴呆高危人群的多领域生活方式随机对照试验中作为替代终点进行了适宜性评估。
本研究为芬兰认知障碍与失能预防干预研究(FINGER)的事后分析,在基线、12 个月和 24 个月(n=1174)时计算 ANU-ADRI。采用最大似然估计的线性混合模型评估 ANU-ADRI 与认知(基线和随时间变化)的相关性、干预对 ANU-ADRI 变化的影响以及基线 ANU-ADRI 对认知变化的干预效果的潜在影响。
较高的 ANU-ADRI 与认知能力较差显著相关,在基线时(例如,全球认知的估计值[95%置信区间]为-0.028[-0.032 至-0.025])和在 2 年的研究期间(例如,ANU-ADRI 的 2 年变化和全球认知的每年变化的估计值[95%置信区间]为-0.068[-0.026 至-0.108])。ANU-ADRI 没有报告出显著的有益干预效果,并且基线 ANU-ADRI 对认知变化的干预反应没有显著影响。
ANU-ADRI 可有效预测认知下降的风险。风险评分可能对新型痴呆症预防策略的成功至关重要,但在为每个环境选择合适的工具时,应仔细考虑其算法、目标人群和干预设计。