Josephs Kennedy A, Josephs Keith A
Department of Neurology, Mayo Clinic, Rochester, MN 55905, USA.
Brain Commun. 2024 Jan 5;6(1):fcae002. doi: 10.1093/braincomms/fcae002. eCollection 2024.
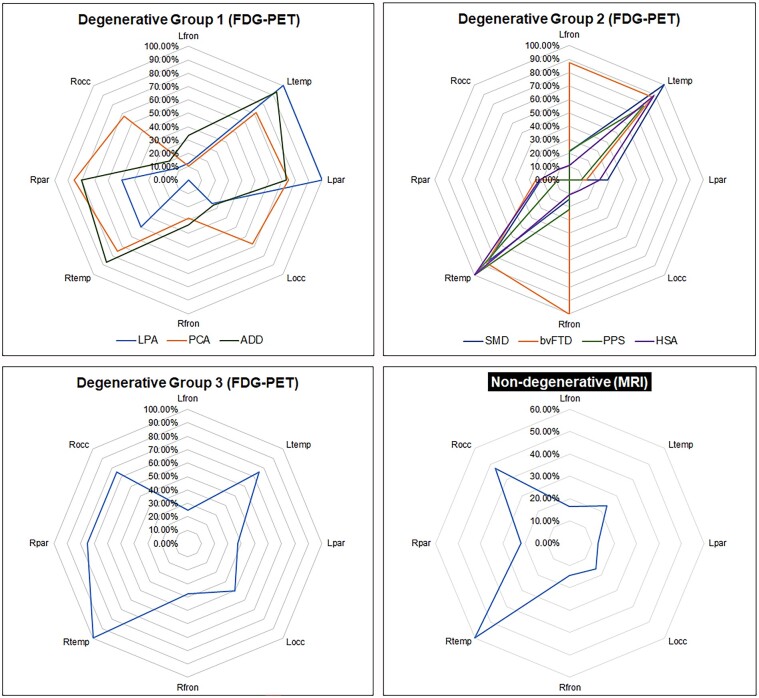
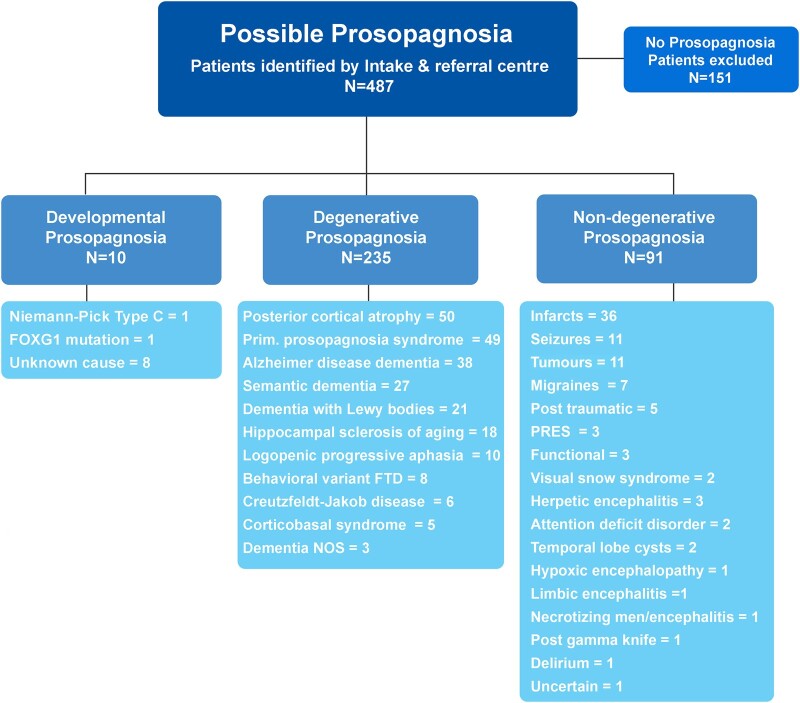
Loss of facial recognition or prosopagnosia has been well-recognized for over a century. It has been categorized as developmental or acquired depending on whether the onset is in early childhood or beyond, and acquired cases can have degenerative or non-degenerative aetiologies. Prosopagnosia has been linked to involvement of the fusiform gyri, mainly in the right hemisphere. The literature on prosopagnosia comprises case reports and small case series. We aim to assess demographic, clinical and imaging characteristics and neurological and neuropathological disorders associated with a diagnosis of prosopagnosia in a large cohort. Patients were categorized as developmental versus acquired; those with acquired prosopagnosia were further subdivided into degenerative versus non-degenerative, based on neurological aetiology. We assessed regional involvement on [F] fluorodeoxyglucose-PET and MRI of the right and left frontal, temporal, parietal and occipital lobes. The Intake and Referral Center at the Mayo Clinic identified 487 patients with possible prosopagnosia, of which 336 met study criteria for probable or definite prosopagnosia. Ten patients, 80.0% male, had developmental prosopagnosia including one with Niemann-Pick type C and another with a forkhead box G1 gene mutation. Of the 326 with acquired prosopagnosia, 235 (72.1%) were categorized as degenerative, 91 (27.9%) as non-degenerative. The most common degenerative diagnoses were posterior cortical atrophy, primary prosopagnosia syndrome, Alzheimer's disease dementia and semantic dementia, with each diagnosis accounting for >10% of this group. The most common non-degenerative diagnoses were infarcts (ischaemic and haemorrhagic), epilepsy-related and primary brain tumours, each accounting for >10%. We identified a group of patients with non-degenerative transient prosopagnosia in which facial recognition loss improved or resolved over time. These patients had migraine-related prosopagnosia, posterior reversible encephalopathy syndrome, delirium, hypoxic encephalopathy and ischaemic infarcts. On [F] fluorodeoxyglucose-PET, the temporal lobes proved to be the most frequently affected regions in 117 patients with degenerative prosopagnosia, while in 82 patients with non-degenerative prosopagnosia, MRI revealed the right temporal and right occipital lobes as most affected by a focal lesion. The most common pathological findings in those with degenerative prosopagnosia were frontotemporal lobar degeneration with hippocampal sclerosis and mixed Alzheimer's and Lewy body disease pathology. In this large case series of patients diagnosed with prosopagnosia, we observed that facial recognition loss occurs across a wide range of acquired degenerative and non-degenerative neurological disorders, most commonly in males with developmental prosopagnosia. The right temporal and occipital lobes, and connecting fusiform gyrus, are key areas. Multiple different pathologies cause degenerative prosopagnosia.

面部识别障碍或面孔失认症已被人们熟知了一个多世纪。根据发病时间是在儿童早期还是之后,它被分为发育性或后天性,后天性病例的病因可以是退行性或非退行性的。面孔失认症与梭状回的受累有关,主要是右侧半球。关于面孔失认症的文献包括病例报告和小病例系列。我们旨在评估一大群被诊断为面孔失认症患者的人口统计学、临床和影像学特征以及相关的神经和神经病理学疾病。患者被分为发育性和后天性;后天性面孔失认症患者根据神经病因进一步细分为退行性和非退行性。我们评估了右侧和左侧额叶、颞叶、顶叶和枕叶在[F]氟脱氧葡萄糖正电子发射断层扫描(PET)和磁共振成像(MRI)上的受累情况。梅奥诊所的接诊和转诊中心识别出487例可能患有面孔失认症的患者,其中336例符合可能或确诊面孔失认症的研究标准。10例患者患有发育性面孔失认症,男性占80.0%,其中1例患有尼曼-匹克C型病,另1例有叉头框G1基因突变。在326例后天性面孔失认症患者中,235例(72.1%)被归类为退行性,91例(27.9%)为非退行性。最常见的退行性诊断是后部皮质萎缩、原发性面孔失认症综合征、阿尔茨海默病性痴呆和语义性痴呆,每种诊断在该组中所占比例均超过10%。最常见的非退行性诊断是梗死(缺血性和出血性)、癫痫相关疾病和原发性脑肿瘤,每种诊断所占比例均超过10%。我们识别出一组非退行性短暂性面孔失认症患者,其面部识别能力的丧失会随着时间的推移而改善或消失。这些患者患有偏头痛相关性面孔失认症、后部可逆性脑病综合征、谵妄、缺氧性脑病和缺血性梗死。在[F]氟脱氧葡萄糖PET检查中,117例退行性面孔失认症患者中,颞叶被证明是最常受累的区域,而在82例非退行性面孔失认症患者中,MRI显示右侧颞叶和右侧枕叶受局灶性病变影响最大。退行性面孔失认症患者最常见的病理发现是伴有海马硬化的额颞叶变性以及混合性阿尔茨海默病和路易体病病理改变。在这个被诊断为面孔失认症的大型病例系列中,我们观察到面部识别能力丧失发生在广泛的后天性退行性和非退行性神经疾病中,最常见于患有发育性面孔失认症的男性。右侧颞叶和枕叶以及相连的梭状回是关键区域。多种不同的病理改变导致退行性面孔失认症。