Zhao Shi, Cao Wangnan, Liao Gengze, Guo Zihao, Xu Lufei, Shen Chen, Chang Chun, Liang Xiao, Wang Kai, He Daihai, Sun Shengzhi, Chen Rui, Dominici Francesca
School of Public Health, Tianjin Medical University, Tianjin, China.
Tianjin Key Laboratory of Environment, Nutrition and Public Health, Tianjin Medical University, Tianjin, China.
BMJ Med. 2024 Mar 6;3(1):e000771. doi: 10.1136/bmjmed-2023-000771. eCollection 2024.
To estimate the association between the transition to daylight saving time and the risks of all cause and cause specific mortality in the US.
Nationwide time series observational study based on weekly data.
US state level mortality data from the National Center for Health Statistics, with death counts from 50 US states and the District of Columbia, from the start of 2015 to the end of 2019.
13 912 837 reported deaths in the US.
Weekly counts of mortality for any cause, and for Alzheimer's disease, dementia, circulatory diseases, malignant neoplasms, and respiratory diseases.
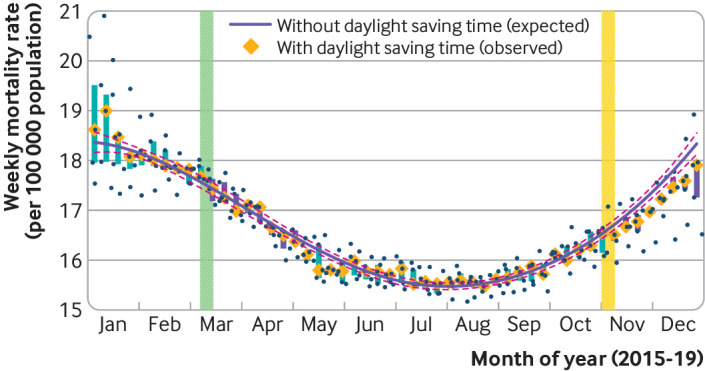
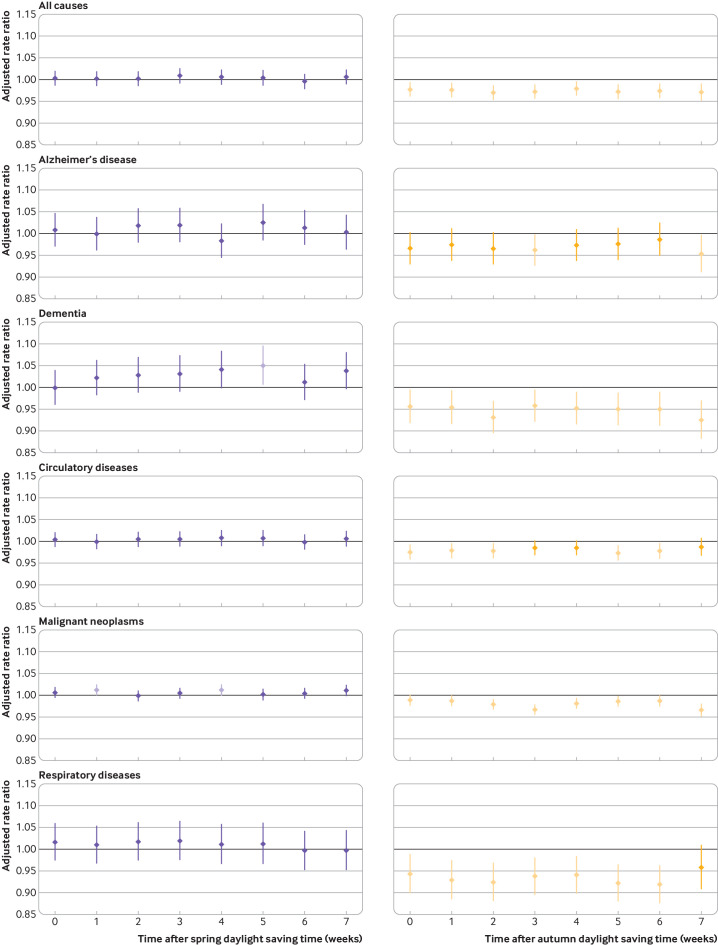
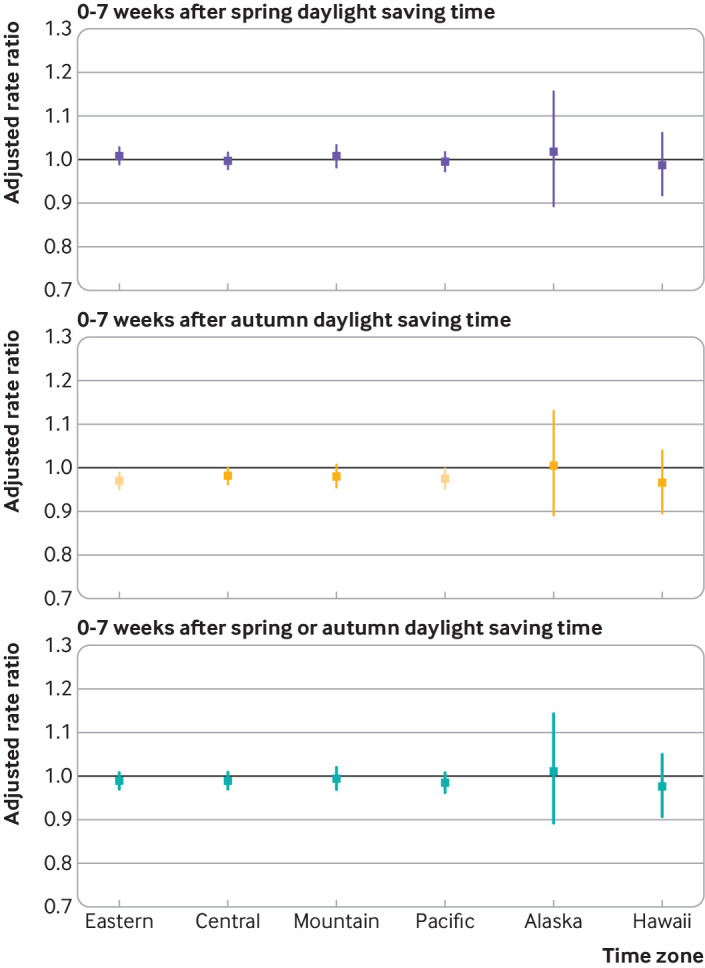
During the study period, 13 912 837 deaths were reported. The analysis found no evidence of an association between the transition to spring daylight saving time (when clocks are set forward by one hour on the second Sunday of March) and the risk of all cause mortality during the first eight weeks after the transition (rate ratio 1.003, 95% confidence interval 0.987 to 1.020). Autumn daylight saving time is defined in this study as the time when the clocks are set back by one hour (ie, return to standard time) on the first Sunday of November. Evidence indicating a substantial decrease in the risk of all cause mortality during the first eight weeks after the transition to autumn daylight saving time (0.974, 0.958 to 0.990). Overall, when considering the transition to both spring and autumn daylight saving time, no evidence of any effect of daylight saving time on all cause mortality was found (0.988, 0.972 to 1.005). These patterns of changes in mortality rates associated with transition to daylight saving time were consistent for Alzheimer's disease, dementia, circulatory diseases, malignant neoplasms, and respiratory diseases. The protective effect of the transition to autumn daylight saving time on the risk of mortality was more pronounced in elderly people aged ≥75 years, in the non-Hispanic white population, and in those residing in the eastern time zone.
In this study, transition to daylight saving time was found to affect mortality patterns in the US, but an association with additional deaths overall was not found. These findings might inform the ongoing debate on the policy of shifting daylight saving time.
评估美国夏令时转换与全因死亡率及特定病因死亡率风险之间的关联。
基于每周数据的全国性时间序列观察性研究。
来自美国国家卫生统计中心的美国州级死亡率数据,涵盖2015年初至2019年末美国50个州及哥伦比亚特区的死亡人数。
美国报告的13912837例死亡病例。
全因死亡率以及阿尔茨海默病、痴呆症、循环系统疾病、恶性肿瘤和呼吸系统疾病的每周死亡人数。
在研究期间,共报告了13912837例死亡病例。分析发现,向春季夏令时转换(3月的第二个星期日时钟拨快一小时)与转换后的前八周内全因死亡率风险之间没有关联证据(率比为1.003,95%置信区间为0.987至1.020)。本研究将秋季夏令时定义为11月的第一个星期日时钟拨慢一小时(即恢复标准时间)的时间。有证据表明,向秋季夏令时转换后的前八周内全因死亡率风险大幅降低(0.974,0.958至0.990)。总体而言,在考虑向春季和秋季夏令时转换时,未发现夏令时对全因死亡率有任何影响的证据(0.988,0.972至1.005)。与夏令时转换相关的死亡率变化模式在阿尔茨海默病、痴呆症、循环系统疾病、恶性肿瘤和呼吸系统疾病中是一致的。向秋季夏令时转换对死亡率风险的保护作用在75岁及以上的老年人、非西班牙裔白人以及居住在东部时区的人群中更为明显。
在本研究中,发现夏令时转换会影响美国的死亡率模式,但未发现与总体额外死亡存在关联。这些发现可能为正在进行的关于夏令时政策的辩论提供参考。