Department of Health and Nursing Science, Faculty of Health and Sport Sciences, University of Agder, Kristiansand/Grimstad, Vest-Agder, Norway.
Marie Curie Palliative Care Research Department, Division of Psychiatry, University College London, London, UK.
Palliat Med. 2024 Apr;38(4):406-422. doi: 10.1177/02692163241238384. Epub 2024 Mar 13.
Shared decision-making is a key element of person-centred care and promoted as the favoured model in preference-sensitive decision-making. Limitations to implementation have been observed, and barriers and limitations, both generally and in the palliative setting, have been highlighted. More knowledge about the process of shared decision-making in palliative cancer care would assist in addressing these limitations.
To identify and synthesise qualitative data on how people with cancer, informal carers and healthcare professionals experience and perceive shared decision-making in palliative cancer care.
A systematic review and metasynthesis of qualitative studies. We analysed data using inductive thematic analysis.
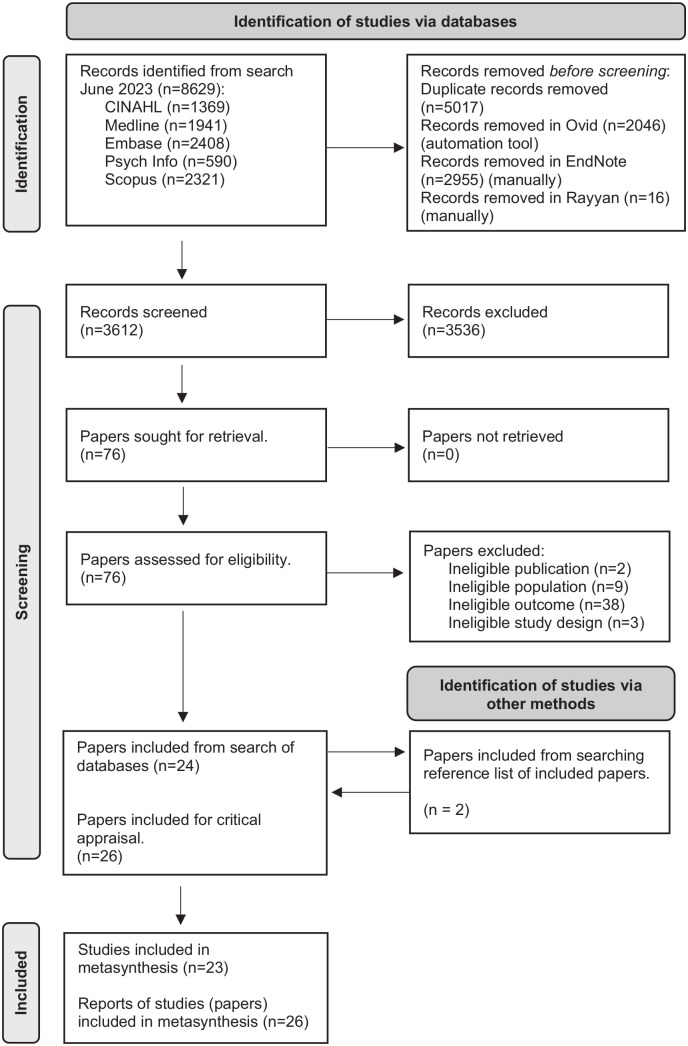
We searched five electronic databases (MEDLINE, EMBASE, PsycINFO, CINAHL and Scopus) from inception until June 2023, supplemented by backward searches.
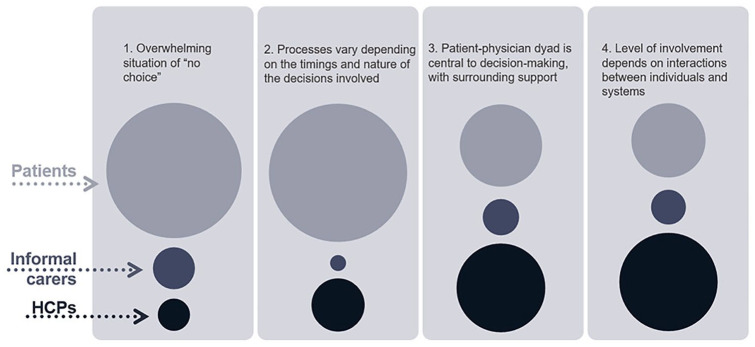
We identified and included 23 studies, reported in 26 papers. Our analysis produced four analytical themes; (1) Overwhelming situation of 'no choice', (2) Processes vary depending on the timings and nature of the decisions involved, (3) Patient-physician dyad is central to decision-making, with surrounding support and (4) Level of involvement depends on interactions between individuals and systems.
Shared decision-making in palliative cancer care is a complex process of many decisions in a challenging, multifaceted and evolving situation where equipoise and choice are limited. Implications for practice: Implementing shared decision-making in clinical practice requires (1) clarifying conceptual confusion, (2) including members of the interprofessional team in the shared decision-making process and (3) adapting the approach to the ambiguous, existential situations which arise in palliative cancer care.
共同决策是以人为本护理的关键要素,被倡导为偏好敏感决策的首选模式。但在实施过程中存在局限性,无论是在一般情况下还是在姑息治疗环境中,都已经凸显出了障碍和限制。更多关于姑息治疗中癌症患者共同决策过程的知识将有助于解决这些局限性。
确定并综合定性数据,以了解癌症患者、非专业护理人员和医疗保健专业人员在姑息治疗癌症护理中如何体验和感知共同决策。
系统回顾和定性研究的元分析。我们使用归纳主题分析对数据进行分析。
我们从开始到 2023 年 6 月在五个电子数据库(MEDLINE、EMBASE、PsycINFO、CINAHL 和 Scopus)中进行了搜索,并通过回溯搜索进行了补充。
我们确定并纳入了 23 项研究,共 26 篇论文。我们的分析产生了四个分析主题;(1)“别无选择”的压倒性局面,(2)决策过程取决于所涉及决策的时机和性质,(3)医患二人组是决策的核心,周围有支持,(4)参与程度取决于个人和系统之间的相互作用。
姑息治疗癌症护理中的共同决策是一个复杂的过程,涉及许多决策,在一个具有挑战性、多方面和不断发展的情况下,平衡和选择受到限制。对实践的影响:在临床实践中实施共同决策需要(1)澄清概念上的混淆,(2)让多学科团队成员参与共同决策过程,(3)根据姑息治疗中出现的模糊、存在主义情况调整方法。