Department of Emergency and Critical Care Medicine, Osaka Medical and Pharmaceutical University, 2-7 Daigakumachi, Takatsuki, Osaka, 569-8686, Japan.
Faculty of Medicine, Osaka Medical and Pharmaceutical University, 2-7 Daigakumachi, Takatsuki, Osaka, 569-8686, Japan.
World J Emerg Surg. 2024 Mar 19;19(1):11. doi: 10.1186/s13017-024-00540-z.
Operative treatment of traumatic rib fractures for better outcomes remains under debate. Surgical stabilization of rib fractures has dramatically increased in the last decade. This study aimed to perform a systematic review and meta-analysis of randomised controlled trials (RCTs) to assess the effectiveness and safety of operative treatment compared to conservative treatment in adult patients with traumatic multiple rib fractures.
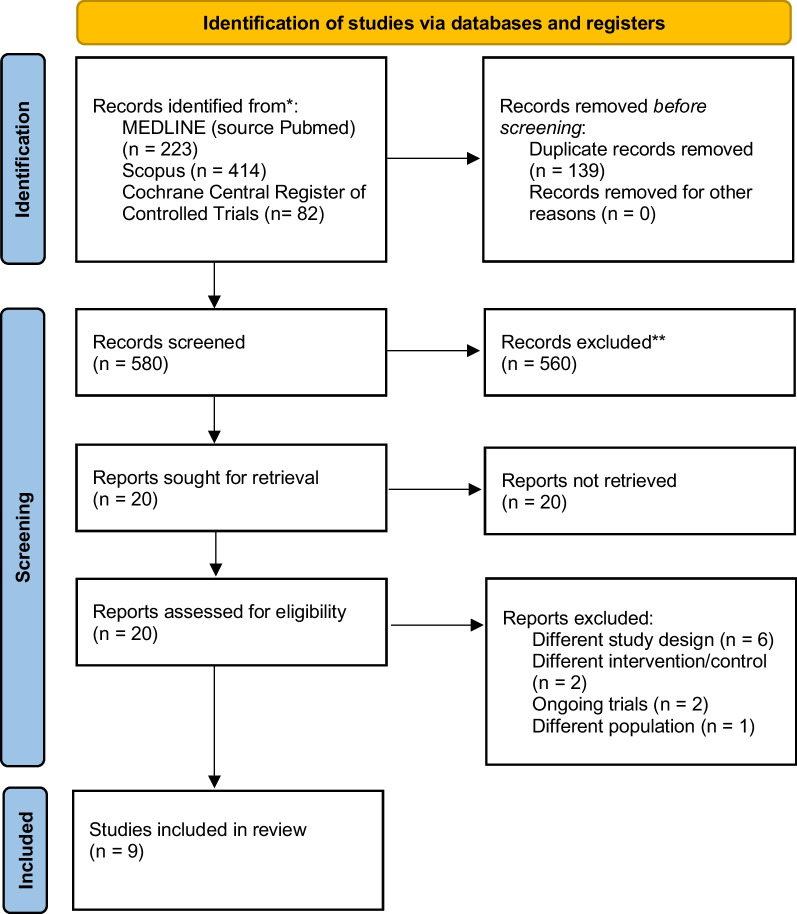
A systematic literature review was performed according to the preferred reporting items for systematic reviews and meta-analyses guidelines. We searched MEDLINE, Scopus, and Cochrane Central Register of Controlled Trials and used the Cochrane Risk-of-Bias 2 tool to evaluate methodological quality. Relative risks with 95% confidence interval (CI) were calculated for outcomes: all-cause mortality, pneumonia incidence, and number of mechanical ventilation days. Overall certainty of evidence was evaluated with the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach, with trial sequential analysis performed to establish implications for further research.
From 719 records, we included nine RCTs, which recruited 862 patients. Patients were assigned to the operative group (received surgical stabilization of chest wall injury, n = 423) or control group (n = 439). All-cause mortality was not significantly different (RR = 0.53; 95% CI 0.21 to 1.38, P = 0.35, I = 11%) between the two groups. However, in the operative group, duration of mechanical ventilation (mean difference -4.62; 95% CI -7.64 to -1.60, P < 0.00001, I = 94%) and length of intensive care unit stay (mean difference -3.05; 95% CI -5.87 to -0.22; P < 0.00001, I = 96%) were significantly shorter, and pneumonia incidence (RR = 0.57; 95% CI 0.35 to 0.92; P = 0.02, I = 57%) was significantly lower. Trial sequential analysis for mortality indicated insufficient sample size for a definitive judgment. GRADE showed this meta-analysis to have very low to low confidence.
Meta-analysis of large-scale trials showed that surgical stabilization of multiple rib fractures shortened the duration of mechanical ventilation and reduced the incidence of pneumonia but lacked clear evidence for improvement of mortality compared to conservative treatment. Trial sequential analysis suggested the need for more cases, and GRADE highlighted low certainty, emphasizing the necessity for further targeted RCTs, especially in mechanically ventilated patients.
UMIN Clinical Trials Registry UMIN000049365.
为了获得更好的结果,对于创伤性肋骨骨折的手术治疗仍存在争议。肋骨骨折的手术固定在过去十年中显著增加。本研究旨在对随机对照试验(RCT)进行系统评价和荟萃分析,以评估手术治疗与保守治疗相比在成人创伤性多发性肋骨骨折患者中的有效性和安全性。
根据系统评价和荟萃分析首选报告项目的指南进行系统文献检索。我们检索了 MEDLINE、Scopus 和 Cochrane 对照试验中心注册库,并使用 Cochrane 偏倚风险 2 工具评估了方法学质量。使用 95%置信区间(CI)计算以下结局的相对风险:全因死亡率、肺炎发生率和机械通气天数。使用 Grading of Recommendations Assessment, Development and Evaluation(GRADE)方法评估证据的总体确定性,并进行试验序贯分析以确定对进一步研究的影响。
从 719 条记录中,我们纳入了 9 项 RCT,共招募了 862 名患者。患者被分配到手术组(接受胸壁损伤的手术固定,n=423)或对照组(n=439)。两组间全因死亡率无显著差异(RR=0.53;95%CI 0.21 至 1.38,P=0.35,I=11%)。然而,在手术组中,机械通气时间(均数差值-4.62;95%CI-7.64 至-1.60,P<0.00001,I=94%)和重症监护病房住院时间(均数差值-3.05;95%CI-5.87 至-0.22;P<0.00001,I=96%)显著缩短,肺炎发生率(RR=0.57;95%CI 0.35 至 0.92;P=0.02,I=57%)显著降低。死亡率的试验序贯分析表明,目前的样本量不足以得出明确的结论。GRADE 表明,这项荟萃分析的可信度非常低或低。
大规模试验的荟萃分析表明,与保守治疗相比,手术固定多发性肋骨骨折可缩短机械通气时间,降低肺炎发生率,但对死亡率的改善缺乏明确证据。试验序贯分析表明需要更多的病例,GRADE 强调了低确定性,强调需要进一步的有针对性的 RCT,特别是在机械通气的患者中。
UMIN 临床试验注册 UMIN000049365。