Garcia Martinez Ana, Lopez-Jornet Pia, Pardo Marin Luis, Pons-Fuster Eduardo, Tvarijonaviciute Asta
Department of Dermatology, Stomatology, Radiology and Physical Medicine, Faculty of Medicine, University of Murcia, Hospital Morales Meseguer Clinica Odontologica Marques Velez S/N, 30008 Murcia, Spain.
Interdisciplinary Laboratory of Clinical Analysis, Interlab-UMU, Regional Campus of International Excellence 'Campus Mare Nostrum', University of Murcia, Espinardo, 30100 Murcia, Spain.
Biomedicines. 2024 May 9;12(5):1048. doi: 10.3390/biomedicines12051048.
Burning mouth syndrome (BMS) is a chronic pain disorder characterized by intraoral burning or dysaesthetic sensation, with the absence of any identifiable lesions. Numerous treatments for BMS have been investigated, though without conclusive results. An analysis was conducted of the efficacy of treatment with a low-level diode laser and clonazepam in patients with BMS, and a study was carried out on the levels of different salivary biomarkers before and after treatment.
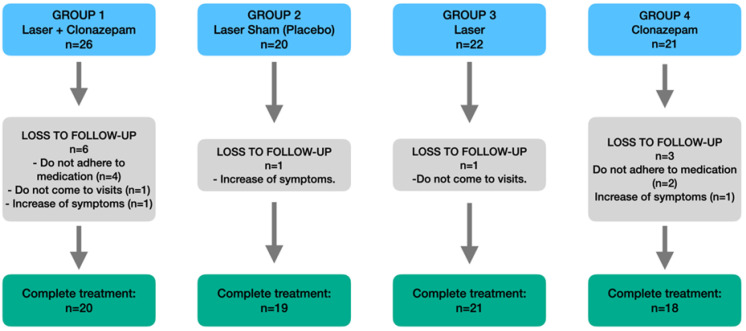
A randomized, single-blind clinical trial was carried out involving 89 patients divided into the following groups: group 1 (laser, The Helbo Theralite Laser 3D Pocket Probe + clonazepam) (n = 20), group 2 (sham laser placebo) (n = 19), group 3 (laser) (n = 21) and group 4 (clonazepam) (n = 18). Symptom intensity was scored based on a visual analogue scale (VAS). Sialometry was performed before and after treatment, and the Xerostomia Inventory, Oral Health Impact Profile-14 (OHIP-14) and Mini-Nutritional Assessment (MNA) questionnaires were administered. The following markers were measured in saliva samples: interleukins (IL2, IL4, IL5, IL6, IL7, IL8, IL1β, IL10, IL12, IL13, IL17, IL21 and IL23), proteins (MIP-3α, MIP-1α and MIP-1β), GM-CSF, interferon gamma (IFNγ), interferon-inducible T-cell alpha chemoattractant (ITAC), fractalkine and tumor necrosis factor α (TNFα).
A significant decrease in the VAS scores was observed after treatment in group 1 (laser + clonazepam) ( = 0.029) and group 3 (laser) ( = 0.005). In turn, group 3 (laser) showed a decrease in the salivary concentration of fractalkine ( = 0.025); interleukins IL12 ( = 0.048), IL17 ( = 0.020), IL21 ( = 0.008), IL7 ( = 0.001) and IL8 ( = 0.007); proteins MIP1α ( = 0.048) and MIP1β ( = 0.047); and TNFα ( = 0.047) versus baseline. Following treatment, group 1 (laser + clonazepam) showed significant differences in IL21 ( = 0.045) and IL7 ( = 0.009) versus baseline, while group 4 (clonazepam) showed significant differences in IL13 ( = 0.036), IL2 ( = 0.020) and IL4 ( = 0.001). No significant differences were recorded in group 2 (sham laser placebo).
The low-level diode laser is a good treatment option in BMS, resulting in a decrease in patient symptoms and in salivary biomarkers. However, standardization of the intervention protocols and laser intensity parameters is needed in order to draw more firm conclusions.
灼口综合征(BMS)是一种慢性疼痛性疾病,其特征为口腔内有烧灼感或感觉异常,且不存在任何可识别的病变。针对BMS已开展了众多治疗方法的研究,但尚无定论。本研究对低强度二极管激光联合氯硝西泮治疗BMS患者的疗效进行了分析,并对治疗前后不同唾液生物标志物水平进行了研究。
开展了一项随机、单盲临床试验,纳入89例患者,分为以下几组:第1组(激光,The Helbo Theralite Laser 3D Pocket Probe + 氯硝西泮)(n = 20),第2组(假激光安慰剂)(n = 19),第3组(激光)(n = 21)和第4组(氯硝西泮)(n = 18)。基于视觉模拟量表(VAS)对症状强度进行评分。在治疗前后进行唾液流量测定,并发放口干症量表、口腔健康影响程度量表-14(OHIP-14)和微型营养评定量表(MNA)问卷。检测唾液样本中的以下标志物:白细胞介素(IL2、IL4、IL5、IL6、IL7、IL8、IL1β、IL10、IL12、IL13、IL17、IL21和IL23)、蛋白质(MIP-3α、MIP-1α和MIP-1β)、粒细胞-巨噬细胞集落刺激因子(GM-CSF)、干扰素-γ(IFNγ)、干扰素诱导T细胞α趋化因子(ITAC)、 fractalkine和肿瘤坏死因子α(TNFα)。
治疗后,第1组(激光 + 氯硝西泮)(P = 0.029)和第3组(激光)(P = 0.005)的VAS评分显著降低。相应地,第3组(激光)治疗后唾液中fractalkine(P = 0.025)、白细胞介素IL12(P = 0.048)、IL17(P = 0.020)、IL21(P = 0.008)、IL7(P = 0.001)和IL8(P = 0.007)、蛋白质MIP1α(P = 0.048)和MIP1β(P = 0.047)以及TNFα(P = 0.047)的浓度与基线相比降低。治疗后,第1组(激光 + 氯硝西泮)的IL21(P = 0.045)和IL7(P = 0.009)与基线相比有显著差异,而第4组(氯硝西泮)的IL13(P = 0.036)、IL2(P = 0.020)和IL4(P = 0.00)与基线相比有显著差异。第2组(假激光安慰剂)未记录到显著差异。
低强度二极管激光是BMS的一种良好治疗选择,可减轻患者症状并降低唾液生物标志物水平。然而,为得出更确凿的结论,需要对干预方案和激光强度参数进行标准化。